
Low-energy summary
- This post uses my own text messages to give a first-person documentary account of an experience of Long Covid and ME/CFS. I use private messages, sent at different times to different people, as a record of crashes, fluctuating symptoms, relapse, remission, pacing, medical uncertainty, and the struggle to make sense of a poorly understood and poorly supported illness.
- The post describes how ME/CFS affects far more than energy. Its many symptoms affect cognition, sleep, pain, movement, digestion, sensitivity, social life, work, and identity.
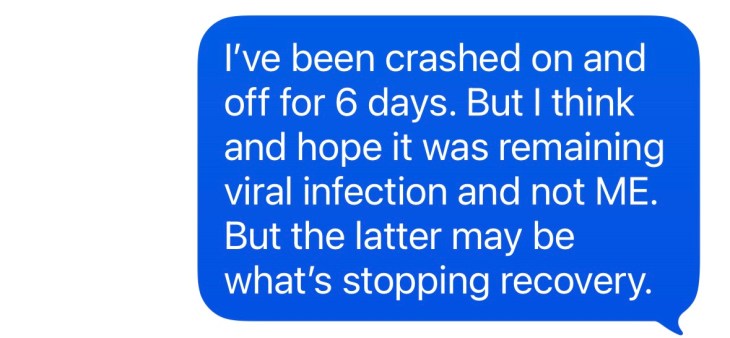
- It also describes the strange unreliability of remission: how feeling better can make the illness harder to remember, and can tempt a return to previous levels of activity, often followed by post-exertional malaise and relapse.
- My own illness has been at the mild to moderate end of ME/CFS, but even this has changed work, identity, relationships, and ordinary life.
- Many people are much more severely affected: housebound, bedbound, dependent on care, and unable to write or advocate for themselves. I am writing partly because I currently can, and partly because many people with severe ME/CFS cannot.
For the last two years, my messaging apps have contained a record that is more reliable than my memory. Short messages, sent to different people at different times, document symptoms, relapses, brief remissions, experiments, medical appointments, and attempts to understand what was happening to me.
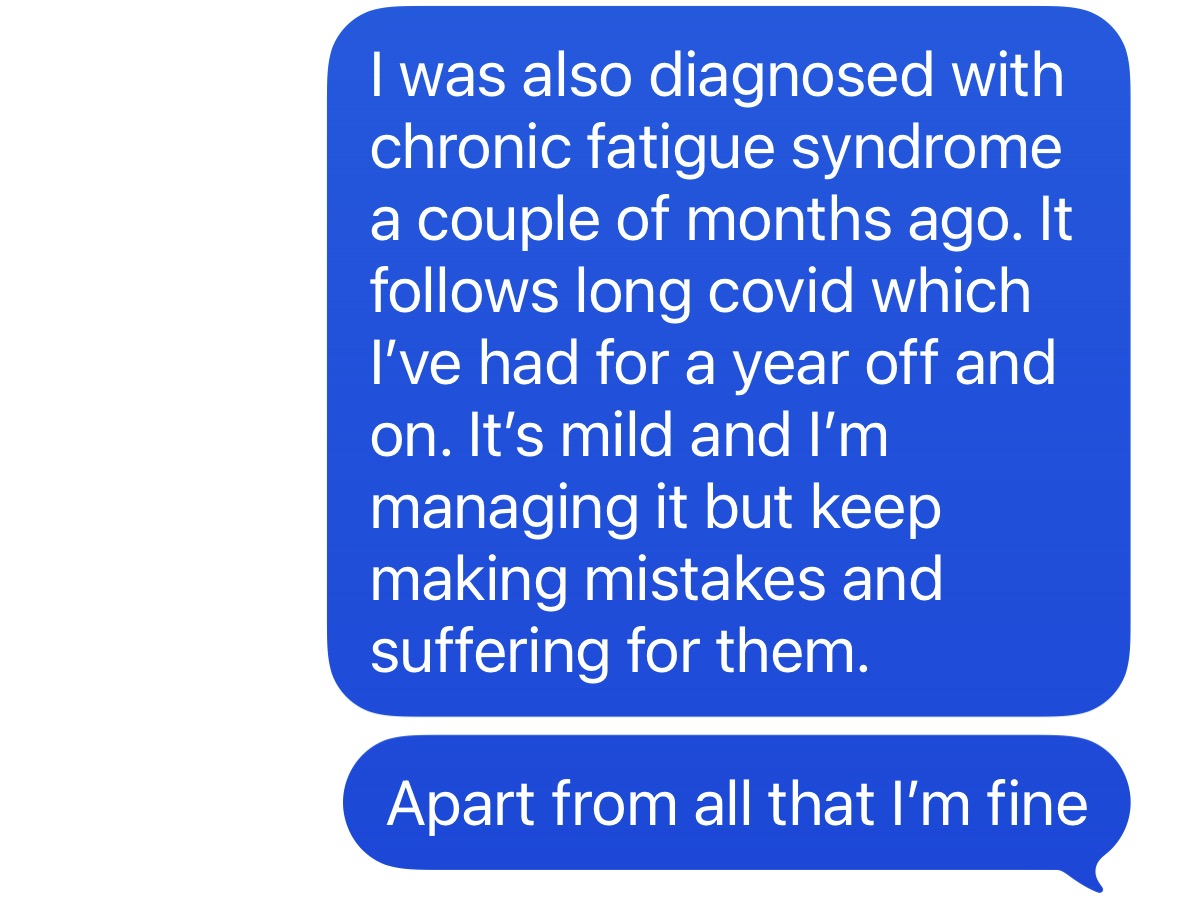
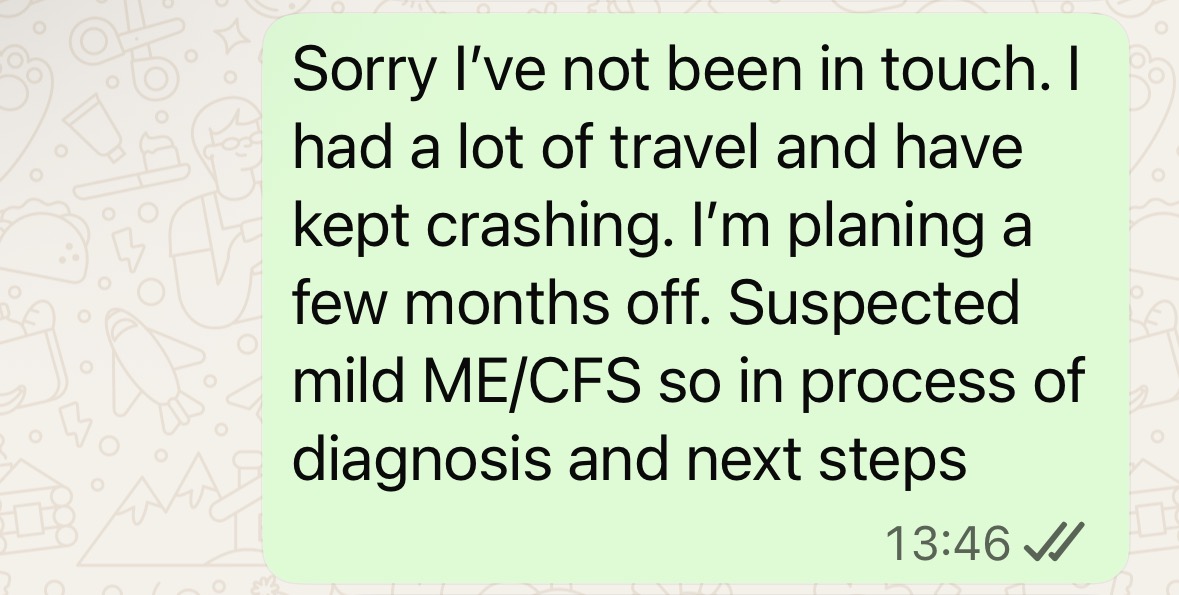
In late 2025, I was diagnosed with Long Covid and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)1. The symptoms followed a Covid infection in summer 2024, though looking back, some had appeared intermittently after shingles (herpes zoster) in 2017. At the time of writing, I am in a period of remission. That is why I can write this. It is also why the text messages are helpful: when I feel better, I find it strangely difficult to remember the patterns of the condition.
This post offers a selection of those messages as a first-person record of a fluctuating, disabling, poorly-understood illness, along with commentary. This is not medical advice. It is a personal account, supported where possible by clinical guidance and research, of how ME/CFS and Long Covid have affected my life and may affect others. The screenshots and message extracts are included as fragments of lived experience, not as clinical evidence.
What is ME/CFS?
ME/CFS1 is a serious, chronic and complex illness, characterised by multiple symptoms, including:
- “feeling extremely tired all the time (fatigue), which can make daily activities like taking a shower, or going to work or school, difficult
- sleep problems, including insomnia, sleeping too much, feeling like you have not slept properly and feeling exhausted or stiff when you wake up
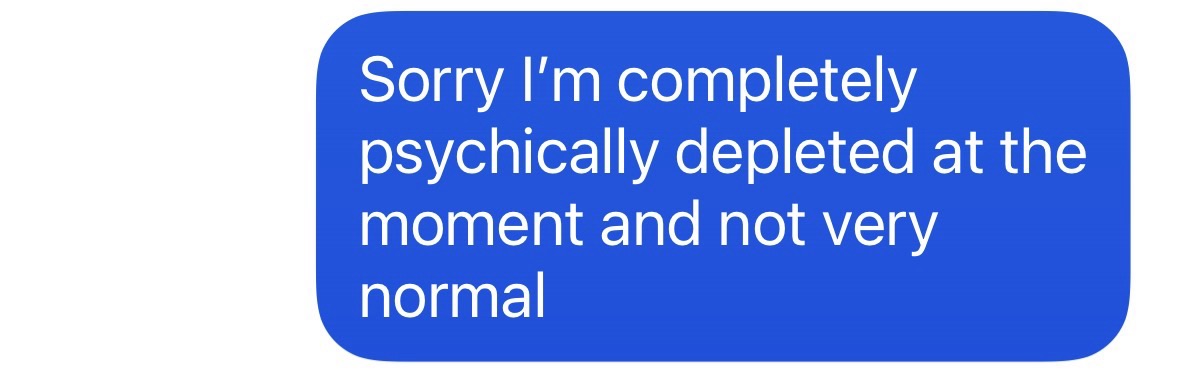
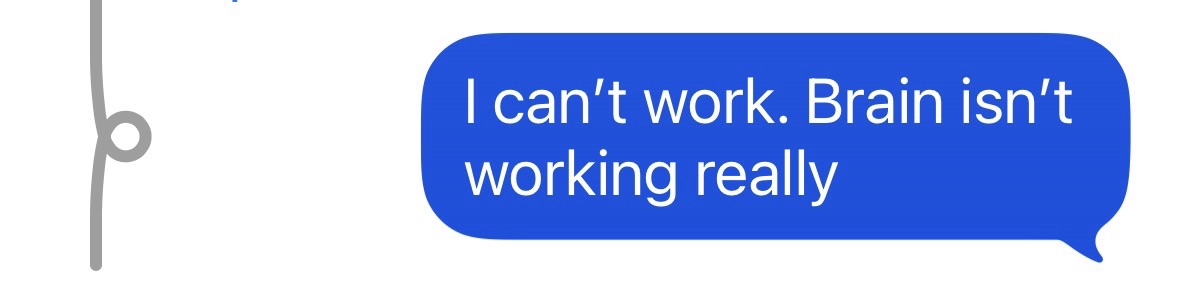
- problems with thinking, concentration and memory (brain fog)
- symptoms getting worse after physical or mental activity, and possibly taking weeks to get better (also called post-exertional malaise, or PEM)” (NHS, 20241)
There are also other symptoms, including pain, flu-like symptoms, dizziness, heart palpitations, muscle twitches or spasms, intolerance to alcohol or certain foods or chemicals, and being very sensitive to light, sound, touch, taste, smell and temperature changes.
The body systems involved are multiple2 and interconnected3. These include the neurological4, immune5, autonomic6, vascular7, metabolic8, and gastrointestinal9 systems.
There are four levels of severity10: mild, moderate, severe, and very severe. To take the two end points, those with mild ME/CFS may still be able to work or engage in education, but probably part-time or with reduced hours, and at the expense of other activities. Light domestic tasks are typically possible, but exertion will be impossible to sustain. At the other end of the spectrum, those with very severe ME/CFS are permanently bedbound and fully dependent on care, to the extent that they may need to be tube fed.
Due to decades of scientific and medical neglect11, historical figures on the number of people affected are hard to come by. But it is estimated that around 400,00012 are affected in the UK, with an estimated global prevalence of 0.89%13, figures that have increased due to the Covid-19 pandemic14.
Many have only vaguely heard of “M.E.” or “chronic fatigue syndrome”. I was one of those people. I didn’t know much more than the primary symptom: profound fatigue. But ME/CFS (the currently accepted term15) is so much more than that, and it is devastating for millions of people, who are missing from society16. Those who really understand ME/CFS are few: those who have experienced it, some of those who have lived with or cared for someone who has experienced it, a very small subset of healthcare workers, and a tiny number of researchers.
I hope that, by the end of this article, you might at least have a better understanding of a devastating and neglected illness.
Fatigue, Crashes, and Post-Exertional Malaise
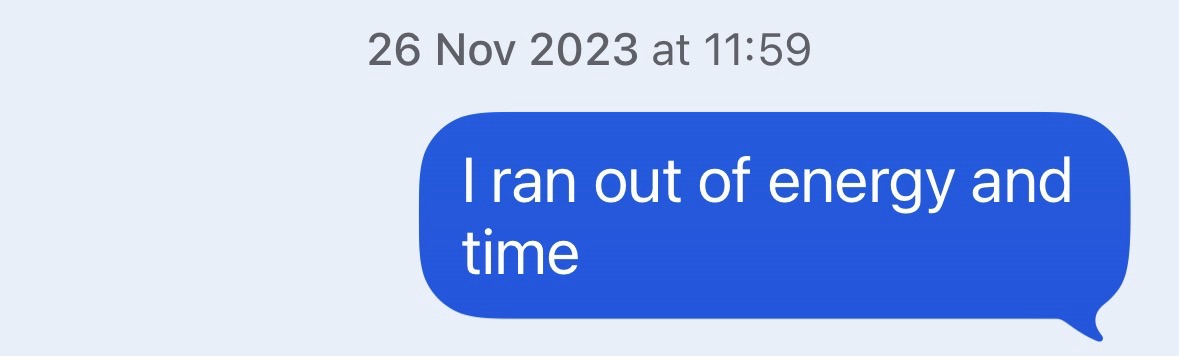
The fatigue of ME/CFS is so unlike the ordinary use of the term, that it feels like far too small a word. It’s not the kind of fatigue one experiences after a workout, a hard day of work, or extensive travel. Even with ‘mild’ ME/CFS, the everyday fatigue of ME/CFS means that ordinary life becomes a huge effort.
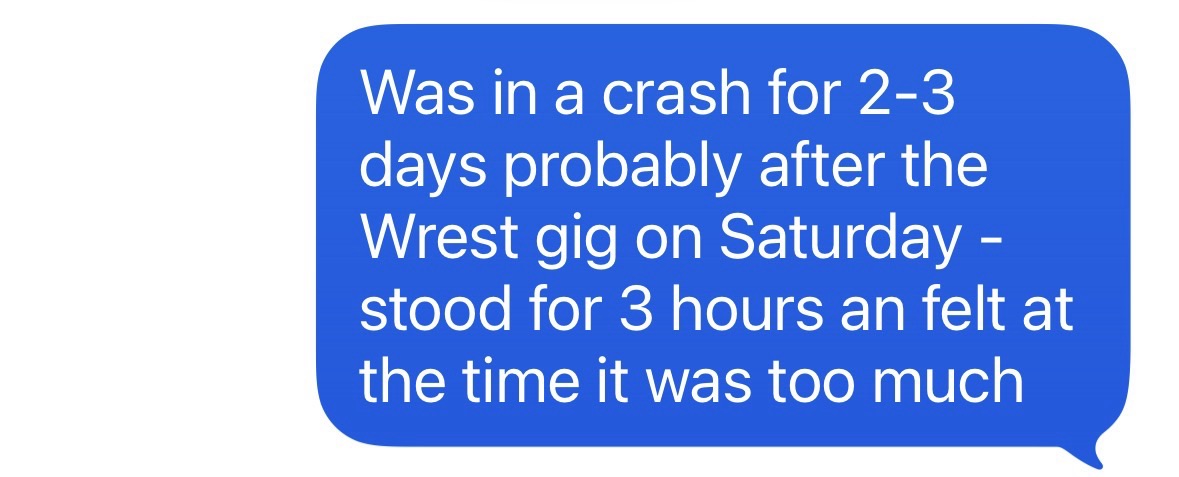
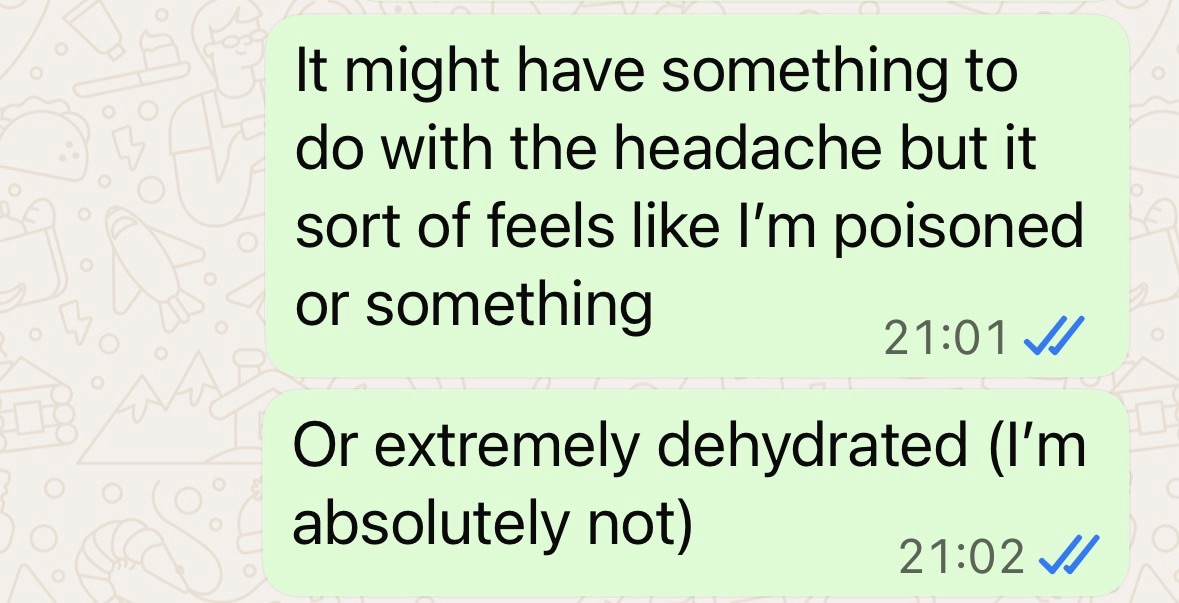
Then there are the crashes. Post exertion malaise (PEM)17 is a defining feature of ME/CFS, and can be thought of as multi-system post-exertional symptom exacerbation (including but not limited to fatigue), the onset of which is typically delayed 12-48 hours18. For me, PEM has a particular feeling of being ‘poisoned’, but a more familiar comparison is described by Belle and Sebastian lyricist and frontman Stuart Murdoch19, who has had ME/CFS for decades: “Sometimes it’s like the worst hangover you’ve had, and you’re going to have it all day and all next week as well.” He added, “And then sometimes it’s like the day before you come down with a bad flu. That sort of feeling that persists and persists”.
PEM can result from exceeding one’s baseline capacity, which may be even trivial physical or mental exertion for those at the more severe end of the spectrum. This is extremely hard to avoid, and learning tends to come at great cost. PEM can result in not only symptom exacerbation, but a dramatic reduction in baseline capacity, which may last days, weeks, months, or even years. Some live in a long-term state of ‘rolling PEM’, where PEM is compounded with a gradual decline in functional capacity, quality of life, and health.




Symptoms Beyond Fatigue
The phrase ‘Chronic Fatigue Syndrome’ is more familiar and easier to recall and use than ‘Myalgic Encephalomyelitis’, but the condition is about much more than chronic fatigue. For me, ME/CFS (at a mild to moderate level) has included:
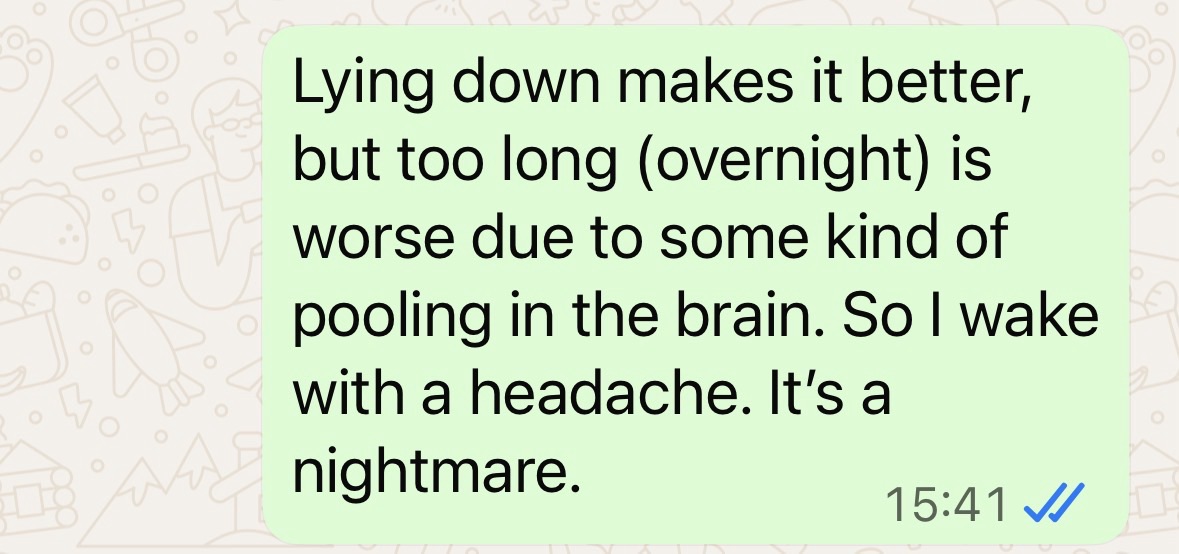
- 24/7 headache and cranial pressure
- body inflammation and pain
- sleep disturbance
- orthostatic intolerance, dizziness, and gait instability
- chronic gut problems
- cognitive dysfunction (‘brainfog’)
- exercise intolerance, wheezing, and shortness of breath
- sensory hypersensitivity
- alcohol intolerance, and
- new cardiac issues.
These symptoms, and more, are common20 for people with ME/CFS and Long Covid. For me, they may arise in any combination, and last for periods from days to months, without break. They can start and end even without any discernible change in behaviour or environment. Some symptoms respond to some interventions, sometimes. But even then, relief tends to be partial. The result is that it becomes difficult to work, socialise, and take care of others (and oneself, for those more severe). Anything resembling a normal life may be impossible.


Remission and Relapse
ME/CFS is a fluctuating condition21, like a game of snakes and ladders. There can be periods of improvement and remission, lasting days, weeks or longer. During these periods, there can be a general reduction in the severity of all symptoms, or symptom-by-symptom improvements, but usually not to pre-illness capacity.
For instance, I’ve experienced symptoms that have lasted for weeks or months, then disappeared, but with other symptoms remaining continuously or intermittently. I’ve also had almost complete remission of all symptoms, with only a growling physiological warning after excessive exertion.
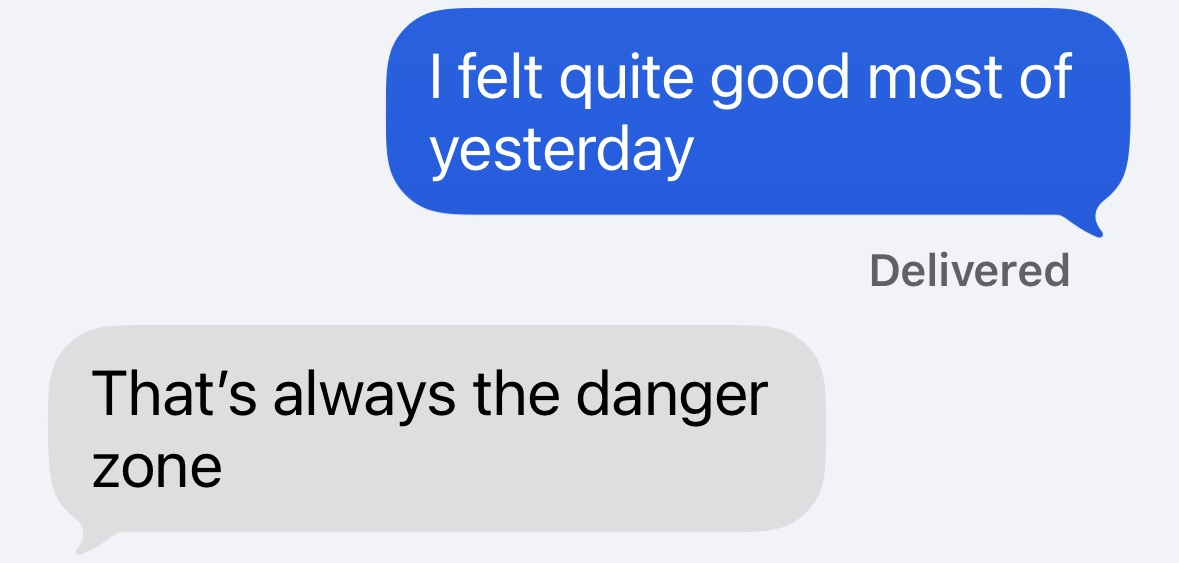
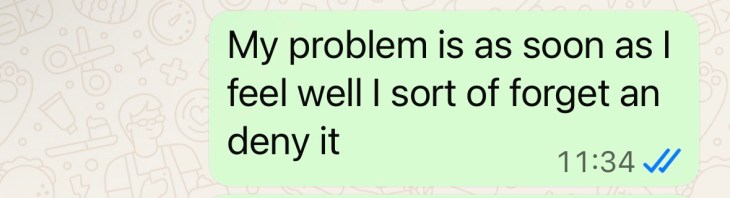
One profound difficulty is that a few days of remission can feel like total remission. It’s happened to me many times, and on every occasion (even as I write) I think I’ve beaten the condition. Feeling able to exert more, without immediately triggering a crash, can almost erase the memory of previous consequences. And so it feels natural to return to near pre-illness levels of activity. For most people with ME/CFS, most of the time, this will result in a very temporary remission. But it brings glimpses of how life used to be, which are both precious and tragic.
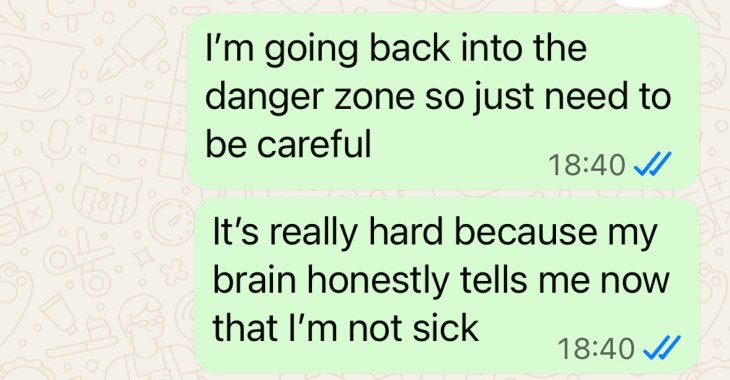
‘Tragic’ because deterioration and relapse22 will nearly always follow, and the snakes seem longer than the ladders. Avoiding deterioration and relapse is a risk management exercise, but the odds are stacked against you. The most common reason seems to be overexertion – exceeding mental or physical limitations. But even with perfect pacing, deterioration can happen after an infection, unavoidable stress or trauma, lack of symptom control, new treatment, surgery, or environmental conditions. In my experience, the first feeling is that familiar poisoned feeling, along with a return of symptoms of profound fatigue and other symptoms in various combinations. None of this is really predictable.
Short-term flare-ups usually last a few days and may be triggered by minor over-exertion or acute stress. These may be resolved with prolonged rest. Longer-term relapses last weeks or months, and require serious, sustained energy management to avoid a new, lower baseline level of functioning. With a reduction in baseline, one may deteriorate through any levels, from mild to very severe.
A very small percentage of people do achieve complete remission. This is thought to be around 5-8%23 of sufferers. Others experience remission for a few months, or even years, only for signs and symptoms to reappear after a new infection, stressor, or period of excessive exertion. Others never experience anything like their former levels of capacity, even for brief periods, and ‘improvement’ may mean being able to eat, dress, or shower unaided, or perhaps take a short walk on a really good day.



Sensemaking
ME/CFS is a confusing condition. It is complex, involving many body systems, physiological processes, and symptoms that interact with each other. The symptoms can have a remitting-relapsing pattern, present and active to different degrees at different times. Within the space of a few days or weeks, the pattern of symptoms can change significantly, making it difficult to impossible to plan. And PEM adds a special confusion of its own via the typical delay of symptoms post exertion; the feedback is delayed, noisy and unreliable, and the consequences of action may not appear until a day or two later.
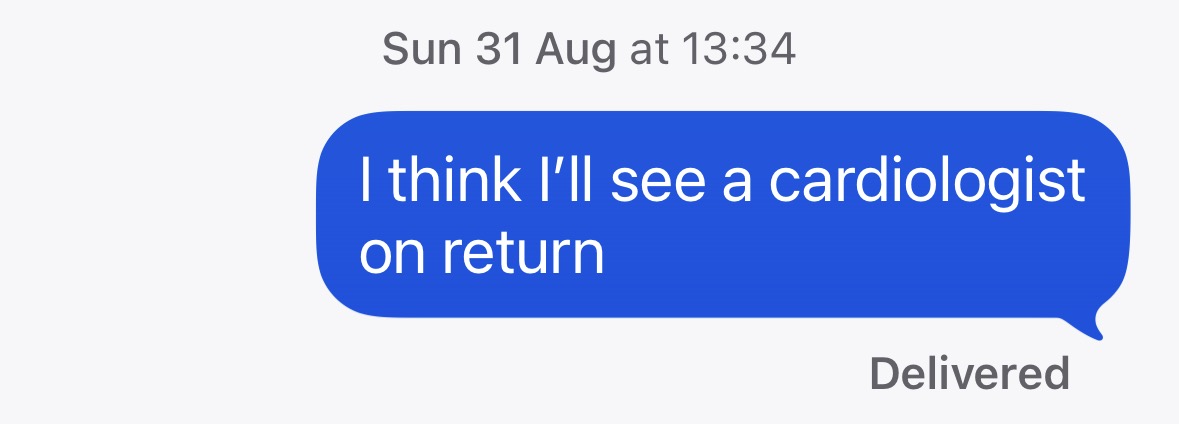
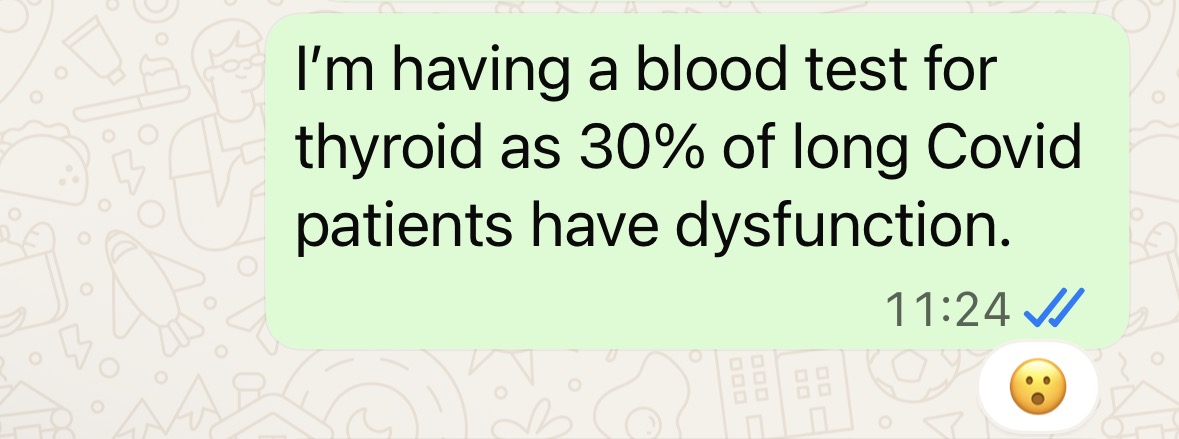
ME/CFS is also known to overlap and interact with other conditions such as postural tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), Ehlers Danlos syndrome (EDS), fibromyalgia, and Long Covid (according to some studies, around half of those with Long Covid meet the criteria for ME/CFS24). Some symptoms may be mistaken for, or may add to, symptoms of such conditions, especially those that feature profound fatigue and pain. To make matters worse, standard medical tests tend to reveal no abnormal results25, and the person may appear normal (the more astute GP will watch how the patient rises from the chair in the waiting room and makes their way to the consultation room, and listen to how they speak). Taken together, these factors make ME/CFS notoriously difficult to make sense of, for patients, families and friends, employers, clinicians, researchers, and institutions such as local government and associated services.
The Medical Maze
ME/CFS is among the most neglected conditions in research and clinical practice. In a British context, research has highlighted that ME/CFS is poorly understood by medical professionals26 with inadequacies in medical school education27. To add to this, relative to its burden, ME/CFS is among the most underfunded conditions in biomedical research28. Clinicians seem to be ill-informed about the complex, multi-system biology of ME/CFS, and relatively few primary care doctors appear to be willing or able to give a diagnosis. And there are often no specialists, since ME/CFS does not belong to any medical specialism.
People with ME/CFS must therefore navigate an exhausting journey to get a diagnosis, sometimes requiring them to travel hundreds of miles to see multiple doctors. Many have to pay for a private doctor even where state healthcare exists, and specialised tests are typically not provided by standard healthcare or covered by insurance.
ME/CFS is diagnosed when symptoms have persisted for three months10 (in a UK context; NICE, 2021), and are not explained by another condition. Many appointments and tests therefore exist to rule out other conditions. For me personally, this has involved scans and tests to exclude – among other conditions – lung disease, bowel disease, heart problems, eye problems, and thyroid dysfunction. Each clinician was looking at only a fragment of the problem, and few appeared to see the whole pattern.
Even after getting a proper diagnosis, there is little good news. The standard medical advice is ‘pacing’ (see later). Some clinicians are willing to prescribe off label for symptom control29, but these clinicians are few. Some patients are given conflicting or even dangerous medical advice (such as ‘pushing through’ or exercise), while others are disbelieved and discharged, or misdiagnosed (with depression, burnout, etc).
For all of these reasons, the most severely ill with ME/CFS are the most neglected. They do not have the capacity, funding or support to navigate all of this. And so they become more sick, and poorer – losing employment and benefits – trapped in a maze with no exit.
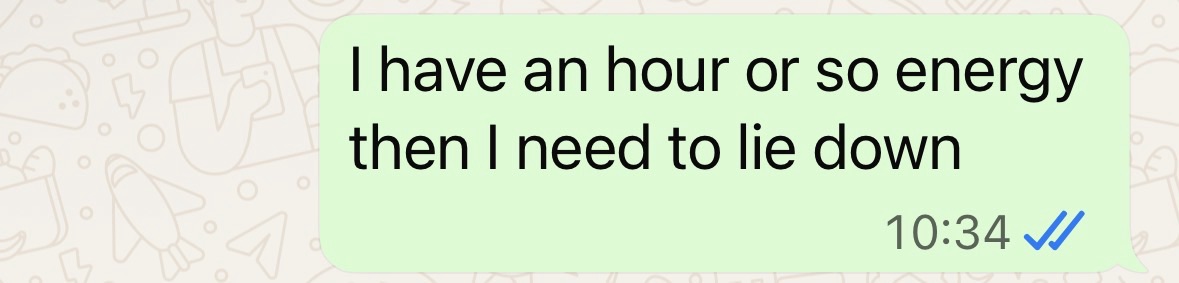
Pacing, Energy Management, and Rest
Pacing30 is a self management strategy involving balancing activity and rest, and moderating exertion, to manage energy and prevent post-exertional malaise (PEM). It means resting before symptoms emerge, not after exhaustion or crashing. Typical approaches to pacing involve breaking tasks down into smaller parts, planning rest breaks, and using data from wearables to avoid overexertion.
In the early stages of post-viral fatigue, before ME/CFS sets in, overexertion is probably the biggest risk. It is important to prioritise rest31 along with pacing activities to facilitate recovery from acute illness. You cannot exercise your way out of ME/CFS, and attempting to do so will almost certainly make things worse. Many patients and clinicians find that overexertion is harmful32. I didn’t rest enough after shingles or Covid, but I can’t know if the illness would have developed anyway.
All of this runs counter to dominant productivity-oriented values and narratives in many western societies, which prize activity and look down on rest. Pacing therefore requires enormous mental strength and discipline. And it requires considerable planning and calculation. Overestimation of what one can do, and underestimation of the time and effort required, seem to be defaults for most people. You have to unlearn your old ways – charging about, people pleasing, over-committing – and get good at pacing. Ironically, you need to do this quickly, before your illness progresses and PEM damage sets in, lowering your baseline.
Most people33 with ME/CFS rely on pacing. Pacing is often the only thing you can really rely on. But every person with ME/CFS will report that there are limits to its effectiveness, and will report making many mistakes, for instance in estimating what one can do, or keeping track of what one has done. And we are not in control of our environment; many things can ruin pacing efforts, including illness or obligations associated with others’ wants and needs. And even if pacing is done perfectly, a person with ME/CFS may still crash, for reasons hidden in the complexity of the condition. While necessary, pacing only prevents one from getting more ill. It does not cure the condition. And other problems – financial, social, mental – still remain. You’re just not getting sicker…hopefully.

Treatments
This section is descriptive, not advisory. It describes the dark, boggy landscape that many patients enter. And to be clear, there are no curative treatments34 for ME/CFS, and none is currently approved by the National Institute for Health and Care Excellence (NICE)35 in the UK (which states “Do not offer any medicines or supplements to cure ME/CFS”). But having a chronic condition often leads a relentless search for treatments such as supplements, medications and other treatments, and various options exist that have been adapted for specific ME/CFS symptoms, with different levels of evidence. Some of these are prescribed by clinicians, while others are a result of personal searches for solutions.
When it comes to supplements, people use a wide variety of options to try to provide mitochondrial and cellular energy support, anti-inflammatory and antioxidant support, gut-immune axis and microbiome modulation, histamine and mast cell stabilisation, electrolyte, mineral, and structural support, and sleep support. This is sometimes on the basis of clinical advice, but often not on the basis of biomedical tests. There is a risk of an ever-growing list of supplements, making it difficult to impossible to know what – if anything – is having an effect. (I routinely take many simultaneously.) If improvements are experienced, it can be impossible to attribute them to any particular intervention or combination. There is also a risk of mistaking placebo effects for mechanistic effects, though if these occur, they are likely to be very early in the illness.
The same is true, perhaps to a lesser degree, for prescription medications for fatigue, pain, orthostatic intolerance, sleep disturbance, cognitive impairment, immune dysfunction, gastrointestinal issues, and associated stress, depression and anxiety. While there is no specific medication for ME/CFS36, some medications are used to manage symptoms, and associated conditions such as mast cell activation syndrome37, often off licence. There are also various non-pharmacological treatments, but again none is specifically approved for ME/CFS or Long Covid in the UK (examples include, but are not limited to, Perrin technique38, transcutaneous auricular vagus nerve stimulation (taVNS)39, transcutaneous nicotine administration40). To further complicate the picture, some treatments may take weeks or even months to affect symptoms, and the relief may not last.
Doubt and the Illusion of Capacity
ME is a physiological illness that has historically been incorrectly framed in psychological terms, at incalculable cost in suffering, loss of life, and loss of living. There is a psychological dimension to living with ME/CFS. It is not that the illness itself is psychological in origin, but that the experience of the illness creates doubt.
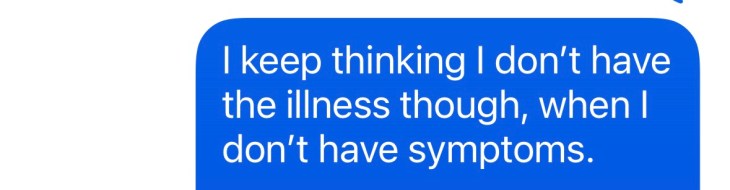
When symptoms improve, when tests are normal, when others do not see what is happening, and when the medical system offers little explanation, it is easy to doubt the illness. “Perhaps I am better now.” “Perhaps I was too cautious.” “Perhaps I can do more.” “Perhaps the crash will not come this time.”
This doubt interacts with an illusion of recovered capacity. At some stages of illness, especially but not only when mild, energy can feel available in a way that seems safe to use. The body appears to give permission to return to normal activity. But for many people with ME/CFS, this can be a false signal. The consequence is post-exertional malaise: a painful and sometimes dangerous reminder that felt energy is not the same as usable capacity.
In time, the baseline level of function (hopefully) returns, and the cycle repeats in roughly the following way:
💭 “Maybe I don’t really have this.”
💭 “I feel like I have some energy.”
💭 “I can use this energy to get things done.”
💭 “I’ve done a normal amount of things, but now I have crashed.”
💭 “I need to lie down and rest, urgently.”
💭 “I feel frustrated, guilty, and foolish because it has happened again.”
💭 “I feel a bit better.”
💭 “Maybe I don’t have this anymore.”
This is a cycle without learning until the consequences of overexertion are bad enough and repeat often enough. But even then, remission of a few days, certainly a few weeks, can feel like total remission. It is almost impossible not to revert to previous patterns when the body feels like it has healed.

A New Reality
At some point, a person with ME/CFS must come to terms with their situation. The alternative may be a progressive or sudden lowering of baseline capacity. There is internal work to be done to come to terms with the diagnosis, create new routines and patterns, and communicate with others. The processes involved can be cyclic, with acceptance and rejection alternating with deterioration and improvement in symptoms. All of this affects not only capacity, but identity. You have to plan and calculate exertion. You have to reduce avoidable stress, while knowing that many sources of stress are not avoidable. You have to say “no” more. You can no longer live like you used to. But how you used to live may have been unsustainable and unhealthy.
What I have found essential is to retain hope. I have never given up the idea that, among the many things that I try, some combination might work, or that my body will be able to recover itself. Each night, before I sleep, I recount everything I’m grateful for about the day, even if that is something small. And when I wake up for a new day, I have hope for how it might go well. I have never, ever lost hope.
But again, I’m one of the ‘lucky’ ones. My form of ME/CFS has meant that I’ve always been able to step outside, and do basic tasks. Others are not so fortunate, and many show forms of endurance that are hard to comprehend from outside.



Why am I writing this?
If you’ve made it this far, and especially if you’ve read previous posts on this blog, you might wonder why I would write this. There are three reasons.
First, I feel safe to do so. Many people with ME/CFS do not feel safe to disclose their diagnosis, as a consequence of negative reactions from clinicians41, family, friends, employers42 or institutions. Despite being a disability covered by law in many countries, ME/CFS is discriminated against socially and institutionally. According to NICE (2021)43 “ME/CFS can cause severe long-term disability, which may be worsened if healthcare workers, relatives, carers, and educational providers/workplaces do not properly recognize the condition and its impact”. I am comfortable to disclose it, whether I am in remission or relapse, partly because I have a level of security that allows me to be comfortable. Many live in a state of economic, social, and health insecurity, which makes disclosure risky and makes the illness worse.
Second, as I have tried to make clear throughout this post, my baseline level has always been ‘mild’ to ‘moderate’. I still have the capacity and ability to self-advocate. Many do not have that; the cognitive dysfunction that comes with ME/CFS has robbed them of their ability to write and self-advocate beyond short posts on social media (e.g., under the hashtag #severeME44). I feel a duty to at least try to advocate for the severely and very severely affected, who remain bedbound. While knowing that I can never understand their situation, I have got to know some with severe forms of the illness, and it’s both infuriating (the injustice and lack of care45) and heartbreaking (the suffering46).
Third, writing is a creative act, and through my worst periods of ME/CFS, small acts of creativity have been essential to my sense of hope and progress. I have had periods of remission where I have written intensively in long form – such as this article on autism47 – and paid for it in the form of relapse. This post has taken longer than usual to write: around three months, in many small acts. I have constructed much of it through gradual curation and sporadic writing. My capability has been unpredictable, so I have had to go with the flow. This is dynamic disability48, where symptoms and limitations fluctuate unpredictably over the long and short term. As I write this sentence, I am in remission. It feels like it could be permanent, but I’ve felt that before…
Can you help?
At the time of publishing this post, we are at the end of ME/CFS Awareness Week49. Unlike diseases such as cancer, diabetes, and heart disease, ME/CFS receives comparatively little research, media attention or even public support. This has begun to change, especially with recent scientific advances in biomedical research, for instance in genetics50 and blood-based biomarkers51.
My brother Gary Shorrock is taking on one of Britain’s most demanding endurance challenges: the Bob Graham Round52 in the Lake District. The funds raised through this challenge will go to ME Research UK53, a charity that commissions and funds high-quality biomedical research into the causes, consequences, and treatment of ME/CFS.
There is an obvious tension in ending a post about energy limitation with an endurance challenge. But that is part of the point. My brother can attempt something that people with ME/CFS cannot imagine doing. He is using that capacity to raise funds for biomedical research into an illness that takes capacity away.
Gary must cover around 66 miles, summit 42 fells, and climb more than 8,200 metres – approximately 26,900 feet of ascent – all within 24 hours. That means steep, rocky, boggy terrain, long hours on the move, and likely sections in darkness and harsh weather. The Bob Graham Round is an exceptional test of endurance, preparation, judgement, and determination. Only around 3,000 people have ever achieved it.
Gary has previously undertaken major endurance events and fundraising challenges, raising over £20,000 for a children’s hospital charity54. Support for this fundraiser will help contribute to urgently needed research into ME/CFS – a devastating and neglected illness. Any donation would be greatly appreciated, and sharing the page would also make a big difference. Please see:
https://www.justgiving.com/page/gary-shorrock, or
Thank you for getting this far, and thank you for your support.
Steven and Gary Shorrock

References
- NHS. (2024, May 28). Myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS). https://www.nhs.uk/conditions/chronic-fatigue-syndrome-cfs/
- Centers for Disease Control and Prevention. (2024, May 10). Clinical overview of ME/CFS. https://www.cdc.gov/me-cfs/hcp/clinical-overview/index.html
- Arron, H. E., Marsh, B. D., Kell, D. B., Khan, M. A., Jaeger, B. R., & Pretorius, E. (2024). Myalgic encephalomyelitis/chronic fatigue syndrome: The biology of a neglected disease. Frontiers in Immunology, 15, 1386607. https://doi.org/10.3389/fimmu.2024.1386607
- Lee, J. S., Sato, W., & Son, C. G. (2024). Brain-regional characteristics and neuroinflammation in ME/CFS patients from neuroimaging: A systematic review and meta-analysis. Autoimmunity Reviews, 23(2), 103484. https://pubmed.ncbi.nlm.nih.gov/38016575/
- Fehrer, A., Windzio, L., Schoening, S., Steiner, S., Aschenbrenner, A. C., Babel, N., Behrends, U., Bellmann-Strobl, J., Cammà, G., Cash, A., Doehner, W., den Dunnen, J., Fluge, Ø., Franke, C., Hoffmann, K., Kedor, C., Kim, L., Löhden, W., Mella, O., Mihatsch, L. L., … Scheibenbogen, C. (2026). Expert perspectives on Myalgic encephalomyelitis/chronic fatigue syndrome – Insights from the 3rd International Conference of the Charité Fatigue Center. Autoimmunity reviews, 25(5), 104043. https://doi.org/10.1016/j.autrev.2026.104043.
- Issa, A., Lin, J.-M. S., Chen, Y., Attell, J., Brimmer, D., Bertolli, J., Natelson, B. H., Lapp, C. W., Podell, R. N., Kogelnik, A. M., et al. (2025). Autonomic dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): Findings from the multi-site clinical assessment of ME/CFS (MCAM) study in the USA. Journal of Clinical Medicine, 14(17), 6269. https://doi.org/10.3390/jcm14176269
- Heng, B., Gunasegaran, B., Krishnamurthy, S., Bustamante, S., Pires, A. S., Chow, S., Ahn, S. B., Paul-Heng, M., Maciver, Y., Smith, K., Tran, D. P., Howley, P. P., Bilgin, A. A., Sharland, A., Schloeffel, R., & Guillemin, G. J. (2025). Mapping the complexity of ME/CFS: Evidence for abnormal energy metabolism, altered immune profile, and vascular dysfunction. Cell reports. Medicine, 6(12), 102514. https://doi.org/10.1016/j.xcrm.2025.102514
- Syed, A. M., Karius, A. K., Ma, J., Wang, P. Y., & Hwang, P. M. (2025). Mitochondrial dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome. Physiology, 40(4). https://doi.org/10.1152/physiol.00056.2024
- Nikolova, R. (2025). Gut microbiome and myalgic encephalomyelitis/chronic fatigue syndrome. International Journal of Molecular Sciences, 27(1), 425. https://www.mdpi.com/1422-0067/27/1/425
- National Institute for Health and Care Excellence. (2021). Myalgic encephalomyelitis/chronic fatigue syndrome: Diagnosis and management: Recommendations (NICE Guideline NG206). https://www.nice.org.uk/guidance/ng206/chapter/Recommendations/
- Sirotiak, Z., & Amro, H. J. (2026). Investigating the ME/CFS experience through qualitative analysis of memorial entries. PLOS ONE, 21(4), e0343374. https://doi.org/10.1371/journal.pone.0343374
- The University of Edinburgh. (2025). ME/CFS cases in England higher than first projected. https://www.ed.ac.uk/news/mecfs-cases-in-england-higher-than-first-projected
- Vardaman, M., & Gilmour, S. (2025). Letter: Time to correct the record on the global burden of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Journal of Translational Medicine, 23, 331. https://doi.org/10.1186/s12967-025-06281-0
- National Institutes of Health. (2025, January 13). NIH-funded study finds cases of ME/CFS increase following SARS-CoV-2. https://www.nih.gov/news-events/news-releases/nih-funded-study-finds-cases-me/cfs-increase-following-sars-cov-2
- American ME and CFS Society. (n.d.). What is ME/CFS? https://ammes.org/what-is-mecfs/
- #MEAction. (n.d.). #MillionsMissing. https://www.meaction.net/millionsmissing26
- Vøllestad, N. K., & Mengshoel, A. M. (2023). Post-exertional malaise in daily life and experimental exercise models in patients with myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Physiology, 14, 1257557. https://doi.org/10.3389/fphys.2023.1257557
- Open Medicine Foundation. (n.d.). Understanding post-exertional malaise (PEM) in ME/CFS. https://www.omf.ngo/pem-in-mecfs/
- BBC. (2018, January 26.). Living with ME is “like being stuck in a waiting room”, says Belle and Sebastian’s Stuart Murdoch. https://www.bbc.co.uk/programmes/articles/3kGdYc1xf2mqRthcHqkbn0p/living-with-me-is-like-being-stuck-in-a-waiting-room-says-belle-and-sebastian-s-stuart-murdoch
- Centers for Disease Control and Prevention. (2024). Signs and symptoms of ME/CFS. https://www.cdc.gov/me-cfs/signs-symptoms/index.html
- MEpedia. (2025, September 3). Fluctuating illness. https://me-pedia.org/wiki/Fluctuating_illness
- ME Association. (2025). Relapses, exacerbations and flare-ups in ME/CFS (Version 2.1) [pdf]. https://meassociation.org.uk/wp-content/uploads/2025/10/RELAPSES-EXACERBATIONS-AND-FLARE-UPS-V2-1.pdf
- Ghali, A., Lacout, C., Fortrat, J.-O., Depres, K., Ghali, M., & Lavigne, C. (2022). Factors influencing the prognosis of patients with myalgic encephalomyelitis/chronic fatigue syndrome. Diagnostics, 12(10), 2540. https://doi.org/10.3390/diagnostics12102540
- Annesley, S. J., Missailidis, D., Heng, B., Josev, E. K., & Armstrong, C. W. (2024). Unravelling shared mechanisms: Insights from recent ME/CFS research to illuminate long COVID pathologies. Trends in Molecular Medicine, 30(5), 443–458. https://doi.org/10.1016/j.molmed.2024.02.003
- Centers for Disease Control and Prevention. (2024). Evaluation of ME/CFS. https://www.cdc.gov/me-cfs/hcp/diagnosis-testing/evaluation-of-me-cfs.html
- Pheby, D. F. H., Araja, D., Berkis, U., Brenna, E., Cullinan, J., de Korwin, J.-D., Gitto, L., Hughes, D. A., Hunter, R. M., Trepel, D., et al. (2021). A literature review of GP knowledge and understanding of ME/CFS: A report from the socioeconomic working group of the European Network on ME/CFS (EUROMENE). Medicina, 57(1), 7. https://doi.org/10.3390/medicina57010007
- Muirhead, N., Muirhead, J., Lavery, G., & Marsh, B. (2021). Medical school education on myalgic encephalomyelitis. Medicina, 57(6), 542. https://doi.org/10.3390/medicina57060542
- Mirin, A. A. (2020). Research update: The relation between ME/CFS disease burden and research funding in the USA. Work, 66(2), 277–282. https://doi.org/10.3233/WOR-203173
- ME/CFS Clinician Coalition. (2021). ME/CFS treatment recommendations (Version 1) [pdf]. Bateman Horne Center. https://batemanhornecenter.org/wp-content/uploads/filebase/Treatment-Recs-MECFS-Clinician-Coalition-V1-Feb.-2021.pdf
- ME Association. (2026). Pacing in ME/CFS (Version 3) [pdf]. https://meassociation.org.uk/wp-content/uploads/2026/02/Pacing-V3.pdf
- Jason, L. A., et al. (2021). A natural history of disease framework for post-viral fatigue syndrome and myalgic encephalomyelitis/chronic fatigue syndrome. Frontiers in Medicine, 8, 688159. https://doi.org/10.3389/fmed.2021.688159
- ME/CFS Skeptic. (2024, April 8.). Exercise and other forms of exertion can cause profound and lasting harm to people with ME. Substack. https://mecfs.substack.com/p/exercise-and-other-forms-of-exertion
- Action for ME. (2025). Big Survey 2019: Impact, pacing, GET and CBT [pdf]. https://www.actionforme.org.uk/wp-content/uploads/2025/01/Big-Survey-2019-imact-pacing-GET-CBT-compressed.pdf
- ME Association. (2025). Treating ME/CFS (Version 2) [pdf]. https://meassociation.org.uk/wp-content/uploads/2025/10/TREATING-MECFS-V2.pdf
- National Institute for Health and Care Excellence. (2021). Myalgic encephalomyelitis/chronic fatigue syndrome: Diagnosis and management: Symptom management for people with ME/CFS (NICE Guideline NG206). https://www.nice.org.uk/guidance/ng206/chapter/Recommendations#symptom-management-for-people-with-mecfs
- NHS. (2024). Treatment: Myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS).https://www.nhs.uk/conditions/chronic-fatigue-syndrome-cfs/treatment/
- Rohrhofer, J. (2025). The clinical relevance of mast cell activation in myalgic encephalomyelitis/chronic fatigue syndrome. Diagnostics, 15(22), 2828. https://www.mdpi.com/2075-4418/15/22/2828
- Riste, L., Perrin, R., Mulholland, T., Hann, M., McDonald, O., & Heald, A. (2026). Testing the Feasibility of a Self-Help Intervention That Includes Lymphatic Drainage to Reduce Fatigue-Related Symptoms Among Patients with Long COVID in General Practice: Experiences from Our Randomized Controlled Trial (RCT). Infectious diseases and therapy, 15(2), 577–589. https://doi.org/10.1007/s40121-025-01287-z
- ME Association. (2026, March 10). Vagus nerve stimulation trial update. https://meassociation.org.uk/2026/03/vagus-nerve-stimulation-trial-update/
- Leitzke, M., Roach, D. T., Hesse, S., et al. (2025). Long COVID—A critical disruption of cholinergic neurotransmission? Bioelectronic Medicine, 11, 5. https://doi.org/10.1186/s42234-025-00167-8
- Blease, C., Carel, H., & Geraghty, K. (2017). Epistemic injustice in healthcare encounters: Evidence from chronic fatigue syndrome. Journal of Medical Ethics, 43(8), 549–557. https://jme.bmj.com/content/43/8/549
- Surendran, G., & Jose, T. P. (2025). Experiences and challenges of staying employed with chronic fatigue syndrome. Discover Public Health, 22, 637. https://doi.org/10.1186/s12982-025-01036-0
- National Institute for Health and Care Excellence. (n.d.). Complications: Myalgic encephalomyelitis/chronic fatigue syndrome. NICE Clinical Knowledge Summaries. https://cks.nice.org.uk/topics/myalgic-encephalomyelitis-chronic-fatigue-syndrome-me/cfs/background-information/complications/
- Nezamdoust, B., & Ruel, E. (2026). Contested and neglected: Social and medical marginalization in severe Chronic Fatigue Syndrome. Social science & medicine (1982), 388, 118766. https://doi.org/10.1016/j.socscimed.2025.118766
- Sirotiak, Z., & Amro, H. J. (2026). Investigating the ME/CFS experience through qualitative analysis of memorial entries. PLOS ONE, 21(4), e0343374. https://doi.org/10.1371/journal.pone.0343374
- Fennell, P. A., Dorr, N., & George, S. S. (2021). Elements of suffering in myalgic encephalomyelitis/chronic fatigue syndrome: The experience of loss, grief, stigma, and trauma in the severely and very severely affected. Healthcare, 9(5), 553. https://doi.org/10.3390/healthcare9050553.
- Shorrock, S. (2026, March 13). Reflections on the autistic spectrum: A critical response to Uta Frith’s views. Humanistic Systems. https://humanisticsystems.com/2026/03/13/reflections-on-the-autistic-spectrum-a-critical-response-to-uta-friths-views/
- The Sunflower Society. (2026, March 23). What is a dynamic disability? https://thesunflowersociety.org/what-is-a-dynamic-disability/
- ME Association. (2026). ME Awareness Week. https://meassociation.org.uk/campaigns/me-awareness-week/
- Gregory, A. (2025, August 6). Scientists find link between genes and ME/chronic fatigue syndrome. The Guardian. https://www.theguardian.com/society/2025/aug/06/genes-me-chronic-fatigue-syndrome
- BBC News. (2025, June 20). Chronic fatigue is not in your head, it’s in your blood – experts. https://www.bbc.co.uk/news/articles/cy8k73443g4o
- Bob Graham 24 Hour Club. (n.d.). The Bob Graham Round. https://www.bobgrahamclub.org.uk
- ME Research UK. (n.d.). ME Research UK. https://www.meresearch.org.uk/
- The Westmorland Gazette. (2023, May 3). Gary Shorrock raises money for Alder Hey Children’s Hospital. https://www.thewestmorlandgazette.co.uk/news/23501665.gary-shorrock-raises-money-alder-hey-children-hospital/
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

I had a friend tell me that this entry was like a dream she forgot to write down- that it explained her. So thank you for teaching me more about my friend and how to be there for her.
LikeLiked by 1 person
Thank you, Leslie. That’s exactly why I wrote it. 💙
LikeLiked by 1 person
Looking forward to more from you.
LikeLike
I’m working on three others on chronic conditions…I should really try to do and finish one at a time but my mind seems to like to work on several jigsaws at once. 😩
LikeLike
Oh, I do that all the time. I have AI hold all of my document structures so that I can freewrite inside them. You don’t have writer’s block when you can just think about something else. I’m a writer, too, if you ever want to “talk shop.”
LikeLiked by 1 person
I also do not mean to hog your attention, but we write about similar things. I have ADHD, Autism, and Cerebral Palsy. Distributed cognition is very helpful with limited working memory, which may be helpful for long COVID brain fog as well. Anyway, the thought just came to me that if you’re into writing about chronic conditions, you might appreciate a technology bent as well.
LikeLike
Many thanks Leslie. I’ll have a look just now. 🙂
LikeLiked by 1 person