
This is the second in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence (this Archetype)
- Taboo
- Ignorance and Fantasy
- Projection
- P.R. and Subterfuge
- Defunct
Each archetype includes a number of examples (currently healthcare-related). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 2: Congruence
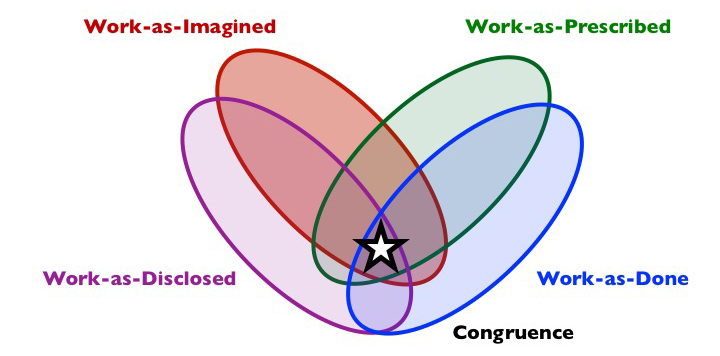
Composition: work-as-done and as-prescribed and usually as-imagined (and often as-disclosed).
Short description: Much human work is done ‘by the book’ – at least in general terms if not the fine detail – and is done much in line with how people who are more removed from the actual work imagine. Such work is often even disclosed, since there is no reason not to. However, prescribed work can have unintended consequences. These, of course, were not imagined, at least by those who designed the work.
What is it?
Congruence comprises activity that largely conforms with prescribed work, and is known to other relevant stakeholders. Congruence might apply to specific activities and where prescription is limited to general goals or principles, essentially giving discretionary space to practitioners. In such cases, work can be said to align with these principles, even though there may be variation in how these are achieved or adhered to. Since work-as-done accords fairly well with procedures and is known to others, it may well be discussed both inside and outside the practitioner group; there is no reason not to, and no reason for P.R. and Subterfuge. Work-as-done in these cases is therefore more or less known and understood further from the sharp end, though this is unlikely to extend far. Congruence will normally reflect quite specific activities, but may resemble much of the work in some environments, e.g., call centres. Much work is likely to shift frequently between Congruence and The Messy Reality.
Why does it exist?
Some work, usually specific activities, can be prescribed such that work-as-done is an accurate reflection of work-as-prescribed. This applies especially where work has a defined process (e.g., simple sequences, loops, or conditional structures [if then <action/s>), where the pre-conditions and conditions of work are more or less known, exceptions are well understood, and variation in system conditions and human performance is restricted and known to relevant stakeholders. In such cases, prescription might be simple or complicated, in the form of procedures, checklists, or forcing functions built into interface dialogues, requiring varying degrees of competence.
In some cases, Congruence may reflect well-designed work, inasmuch as the imagination of how it will and should be done matches how it is and should be done in order to optimise system performance and human well-being. There is typically a high level of field expert involvement in the design of this kind of work (including resources and constraints), for instance via a human-centred design processes. In other cases, how work is done informs how work is prescribed and imagined, i.e., procedures are written to reflect the real work. Here it may be the case that there is a low authority gradient or power-distance, and management is well connected to the front-line work.
A technological forcing function (also known as a poka-yoke), such as a hard interlock on a chemical processing plant or a required field on a web form, may ensure that work is done in the way that it is prescribed, with no or few opportunities for variation. This is likely to reflect specific activities rather than the general work. In other cases, organisational monitoring and control systems (e.g., audits, competency checks, behaviour-based safety), and associated sanctions, may ensure that work is done in the way that it is prescribed. In such cases, the way that people talk about the work is also likely to conform with how it is done at that time, leaving those further removed from the sharp end with a perception of Congruence, which may be persist only for a time…
Shadow side
Work-as-prescribed may be badly designed, such that it is inefficient or even hazardous, e.g., conflicting air traffic control arrival and departure routes designed by someone with no experience of working the airspace. In such cases, work may be done in the way that it is supposed to be done, and this may be known, but the hazards may not be known, especially beyond the front-line. In some such cases, prescribed work may not account for exceptional ‘black swan’ events that are beyond the imagination of those who prescribed the work. An example of this is the checklists in QF32 (2010). In this case, multiple aircraft system failures resulted in dozens of electronic centralised aircraft monitor (ECAM) alerts, which could not be processed by the crew in the prescribed way, forcing them deep into The Messy Reality, which was never imagined (i.e., never projected). In this case, and in the better known Hudson River landing (2009), the crew had very high levels of competence. In other cases, lack of competence or experience may leave practitioners unaware of how to anticipate, detect, and handle such trip hazards. On a social level, group processes may be at play. Prescribed work may be hazardous, inefficient or otherwise ineffective, but people may become desensitised to this by the need for group cohesion and harmony, fear of speaking up or rocking the boat, or may have attempted before, but given up.
Where work-as-done is monitored and controlled, especially where work is not well designed, and in a climate of low trust, Congruence may emerge only temporarily. Typically, this cannot be sustained for long due to the variable and degraded nature of real (as opposed to imagined) system conditions (goals, demands, pressure, resources, constraints, incentives, punishments, climate, etc.), which force a return to the The Messy Reality when monitoring and control allows. Those observing work-as-done, however, may leave with the impression that Congruence is the norm.
Examples (Aviation)
(New examples are added to the top)
Open reporting. I submitted and ASR (Air Safety Report) as mandated following a Missed Approach that could have been avoided had I picked up on certain cues. The outcome was safe but I wanted to take a closer look at the detail. Recordings of the flight instruments on approach were made available to me and I was able to discuss the event with an experienced ‘guardian’ pilot, in confidence, with no fear of recrimination or blame. The whole experience played out exactly ‘as prescribed’. Most pilots are happy to report incidents “by the book” because they see it as a trustworthy process and appreciate its value. I am in no doubt that it could not exist in a blame culture.
Anonymous, Professional Pilot
Flight Plans: Computer-generated flight plans are incredibly accurate. On modern aircraft actual flight time and fuel data can match the plan almost exactly, to the predicted minute and fuel burn. Deviation may be required for weather or unforeseen events but in normal circumstances pilots do the work exactly as prescribed and follow the plan to the letter.
Anonymous, Professional Pilot
SOP’s: I’ve been flying for over 20 years now and still marvel at the power of SOP’s. Effectively, two pilots who have never met before can perform seamlessly on a flight, with each knowing what the other is going to say and do in any given moment. SOP’s enable us to carry out our normal day to day work safety and consistently ‘by the book’ so most pilots are diligent in applying them. They can however become ‘defunct’ or part of the ‘messy reality’ in ‘non-standard’ conditions which demand adaptive responses.
Anonymous, Professional Pilot
Examples (Healthcare)
(New examples are added to the top)
The administration of controlled drugs is done by two competent practitioners, following a clear written policy. There is strict adherence to policy and any deviation would be reported and investigated.
When working at the NHS Litigation Authority (now called NHS Resolution) we undertook a study of the risk management assessments that organisations were required to complete in order to belong to the litigation scheme. NHS organisations would be assessed by trained assessors who would look at the documentation, talk to staff and make judgements on whether they were a level 1, 2 or 3 (1 being compliance against the standards – 3 being sustained and embedded activity).
The review showed:
- for a short window of time the organisation kept clear records of training, improved their documentation and information giving for patients and conducted risk assessments whenever appropriate as well as all sorts of other expectations from these standards
- this performance only lasted for the time of the assessment and it appeared impossible for the organisation to keep it up over time
- there was an extraordinary amount of resource (people, time, money, effort) put into getting ready for an assessment and during the assessment process – some of the people who provided full time work to this were doctors and nurses taken off their clinical roles to help
- there appeared to be no correlation between the level the organisation was at and their actual safety.
We decided to abolish the assessment process.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
In general, most new guidelines published place a greater burden on imaging services as early diagnosis of a particular condition means fewer repeat hospital/GP attendances. Usually many ‘normal’ scans are performed to catch a few abnormalities. Lumbar spine MRI and cancer investigation/follow up are examples.
Anonymous, Radiologist
I work with someone who sticks rigidly to protocols and rules, even when factors like time pressure and other members of staff trying to ‘get ahead’ exist, this staff member has a thorough approach that sometimes causes friction amongst the team. However, as their manager, I value this member of the team as I know they adhere to policies, that their attention to detail and quality of work is always very high, and that there presence in the team is brilliant because it causes those around them to maintain high standards and not ‘cut corners’, which in turn could lead to incidents.
Anonymous, Radiographer
Congruence can happen in the medical workplace, but is usually not the norm. An example would be the use of debriefing after a day’s operating list. A debrief should take place at the end of every team’s operating list, and has been mandated in Scotland for a number of years. In my operating theatre we do have a debrief at the end of every list. Work is therefore ‘congruent’ – our work-as-done is identical to work-as-prescribed (mandated by the Scottish patient safety programme) and we perform a robust, checklist-prompted debrief looking at both task and team performance, so our work-as-done is also congruent with work-as-imagined (in some teams a very superficial debrief occurs – so work-as-done technically is congruent with work-as-prescribed; a debrief does take place – but is certainly far removed from work-as-imagined). As a result we also have a positive attitude to work-as-disclosed – as we are very happy to talk about implementing a process that we feel quite proud of. We are however, a positive outlier in this respect – and finding Congruence in this domain is the exception rather than the norm.
Craig McIlhenny, Consultant Urological Surgeon, @CMcIlhenny
One of the priority areas for the Scottish Patient Safety Programme in Primary Care (SPSP-PC) was the accurate reconciliation of changes to patients’ medication regime following discharge from hospital. The use of a care bundle audit was promoted to measure compliance with a number of process measures, including completing the reconciliation within a set time frame and discussing significant changes with patients or carers. This has many potential benefits especially as patients are vulnerable to medication-related harm (due to inappropriately prescribed or omitted medication) after discharge. In my practice, systems were altered to ensure compliance with the bundle audit and 100% compliance was quickly achieved. This may seem like success but a few problems arose. Staff prioritised contacting patients to discuss medication changes whereas previously they knew which patients were confused about their medication and would contact the pharmacy (rather than the patient) to make sure changes were implemented. This resulted in delay in implementing changes, increased confusion for patients and more work for staff. Secondly, the information in the immediate discharge letter (IDL) is often inaccurate. With the focus on accurate reconciliation, any discrepancy between the immediate discharge letter (IDL) and the patient’s pre-hospital medication list had to be resolved. This meant changing the patient’s usual medication list if the information on the IDL seemed reasonable. However, if there was no obvious justification for discrepancies, clarification would be sought from secondary care. This would delay the process of completing medicines reconciliation and increase work for staff in both primary and secondary care. Previously GPs would often make changes to the patient’s usual medication list based on their knowledge of the patient, their condition and the information from secondary care.
Duncan McNab, GP, @Duncansmcnab
A Do Not Attempt Resuscitation (DNAR) form is put into place when caregivers feel that resuscitation from cardiac arrest would not be in the patient’s best interests. These forms have received a significant amount of bad press, primarily because caregivers were not informing the patient and/or their families that these were being placed. Another problem with DNAR forms is that some clinicians feel that they are being treated as “Do Not Treat” orders, leading (they feel) to patients with DNAR forms in place receiving sub-standard care. This means that some patients who would not benefit from resuscitation are not receiving DNAR forms. As a result when these patients have a cardiac arrest they are subjected to aggressive, yet ultimately futile, resuscitation measures which may include multiple broken ribs, needle punctures in the arms, wrists and groin, and electric shocks. It is not unusual to hope that these patients are not receiving enough oxygen to their brains to be aware during these last moments of their lives.
Anonymous, Anaesthetist
Most hospital pharmacy departments in the UK now use dispensing robots for a large chunk of their medication dispensing. Robotic dispensing reduces the risk of picking errors (manually picking the wrong item from the shelf), as well as theoretically speeding up the dispensing process. Though the overall process may vary depending on whether other systems are electronic or manual (e.g. paper prescription charts or an electronic prescribing system), the work-as-imagined/as-prescribed is along the lines of: operator enters prescription details into pharmacy computer system, indicating the required item; computer system communicates with robot; robot picks correct item from shelf and outputs it to the operator for labelling and checks. For much of the time this process accurately reflects the work-as-done (by human and robot), and the process works very well. However, there are occasions when things can go wrong. An example: a request is received for an antibiotic injection (clindamycin); it is showing up as out of stock on the pharmacy stock control system, but the robot inventory indicates the item is there. In order to supply the item, the operator uses the stock control system to create a label for the clindamycin injection (which is still as-prescribed), and then walks round to the back of the robot to perform a manual output of the item. However, they may manually output a different antibiotic injection (clarithromycin) inadvertently, and dispense this in error, with the clindamycin label. The automated robotic picking system has been bypassed, removing that safety net.
Anonymous, Pharmacist
As I walked into the six bedded bay the patient in the first bed on the right was in distress and breathing heavily. He looked very frail. I was on my ward round with a long list of patients to see with our team of doctors. We went to the middle bed on the right, drew the curtains around and attended to our patient. During the consultation there was a commotion from the next bed and a Cardiac Arrest call was put out. The patient was put on the floor, chest compressions and ventilation started (Cadio-pulmonary resuscitation, CPR) whilst we waited for the Resuscitation Trolley to arrive along with the full Cardiac Arrest team. The nurse read out the patient’s notes and we immediately stopped the CPR attempt, and the patient was pronounced dead. The patient had been in frail health with advanced chronic obstructive pulmonary disease (COPD), heart failure, kidney impairment and had been chair bound at home. Overnight the admitting Doctor had written “Discuss DNACPR (Do Not Attempt Cardiopulmonary Resuscitation) with the Consultant in the morning”. Instead of dying with symptoms of breathlessness controlled by morphine and oxygen and having a Health Care Assistant sit with him as be died, he was left with distressing breathlessness. Then we did chest compressions and ventilation as he died. We did not get as far as using the defibrillator. I am sure that the chest compressions would have been forceful enough to break some ribs. In this scenario it is possible that the patient had some consciousness, and that his last memories would have been fear and pain. The other patients in the bay were, of course, terrified by these events and no one in the healthcare team felt good about the turn of events. Looking back I feel guilty that I did not turn to that patient, and take steps to ensure he had a calmer end of life.
What is sad is that this is not an unusual story. Unless a person dying in Hospital or a Nursing Home has a DNACPR then CPR will be usually be done. CPR may even be done when a person in frail health dies at home without a DNACPR, because the paramedics may be instructed to do CPR ”Just in case it was a cardio-pulmonary arrest”. Nurses and paramedics work in such fear of not doing CPR when there is no DNACPR that they may override their own professional judgement and do CPR when it is clearly inappropriate. Recently a nurse was reprimanded by the Nursing and Midwifery Council for not trying CPR on a nursing home resident who, in my opinion, was clearly already dead. I know of a case in our Hospital in which CPR was started on a person whose body was already in rigor mortis.
How did we get to this point in the United Kingdom that to ensure a person experiences a calm end of life, a DNACPR form must have been completed, and be available in a prominent place? Unless the DNACPR is readily available to the compassionate nurse, instead of comforting the dying person with her presence, her touch, words of kindness and symptoms relieving medicine, instead she must start basic life support and call for a Cardiac Arrest Team?
Dr Gordon Caldwell, Consultant Physician, @doctorcaldwell
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts