
This is the fourth in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence
- Taboo
- Ignorance and Fantasy (this Archetype)
- Projection
- P.R. and Subterfuge
- Defunct
Each archetype includes a number of examples (currently healthcare-related). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 4. Ignorance and Fantasy
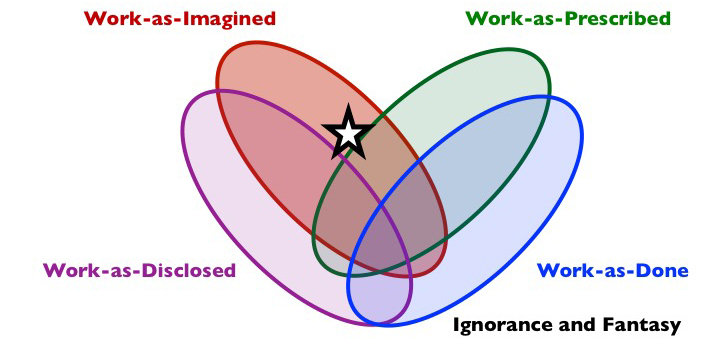
Composition: work-as-imagined, often as-prescribed but not as-done (may or may not be as-disclosed).
Short description: This is what people don’t know about real work and what they imagine happens. The imagination relate to official policy, procedure, standards, guidelines, etc that people assume are in force, or there may just be a general impression of how things work and should work. The primary focus of Ignorance and Fantasy is the imagination of those removed from the actual work.
What is it?
The Ignorance and Fantasy archetype concerns work-as-imagined, usually in the minds of those who are more distant from the work, who often lack knowledge about how things work, perhaps imagining that work is a reflection of what is actually prescribed. Ignorance and Fantasy may be harmless, but if it is disclosed inappropriately in verbal or written form (e.g., to those who can invalidate it or hold people to account for it), or if it is the basis of decisions about the actual work (e.g., demand, resources, constraints), then it may be harmful. As it applies to current work, Ignorance and Fantasy will tend to apply more to some policy makers, journalists, senior managers, other professions (who do not do the work), and the public. Ignorance and Fantasy may occasionally apply to those who actually do the work, when those people have an imagination about how they work (or would have worked) which is not how it is really done – a fantasy. We may genuinely think and declare that we do work one way but actually do it another way. Ignorance and Fantasy inhabits a different zone to The Messy Reality, and if the two ever come into contact there can be surprise, bewilderment, even outrage…and more mess.
Why does it exist?
Most of those who exhibit the Ignorance and Fantasy archetype are far removed from work-as-done and those who do the work, or lack understanding of it, or both. Lack of knowledge and understanding is therefore a primary reason for the existence of archetype. A group who knows little about the real work may reinforce shared beliefs about the work: false consensus.
There may be several perceived benefits to Ignorance and Fantasy. A false narrative about the work may reduce the perceived need to really understand The Messy Reality, which is often difficult to understand. It can also reduce uncertainty, confusion and anxiety about how we think others work. There can be significant cost savings, because Ignorance and Fantasy can negate the perceived need to spend resources to properly understand or improve work-as-done (including the system conditions under which work is done). For journalists and the public, Ignorance and Fantasy offers an easy to understand narrative which helps to reduce uncertainty and gives a simple explanation for events that mask context, complexity and causation (e.g., ‘human error‘ or hero/villain narrative).
Shadow side
As mentioned above, Ignorance and Fantasy can be harmless. Most people do not need to know much, or even anything at all, about various types of work-as-done. We may not, however, want to know about the details of work-as-done (when we really ought to know) in light of the consequences of this knowledge for us. As said by Iris Murdoch (Irish-British novelist and philosopher): “We live in a fantasy world. A world of illusion. The great task is to find reality. But given the state of the world, is it wise?”.
But Ignorance and Fantasy, whether through simple lack of knowledge or not wanting to know, can also be extremely harmful, and lead to problematic decisions, or inaction. At a management or regulatory level, this may concern, for instance, staffing, training, and equipment, and constraints such as rules and regulations or goals such as performance targets. There can be problems of risk control, accountability and liability. Various means of organisational monitoring, assessment and control – including risk assessments and resulting risk controls – may be relied up yet rendered impotent, essentially Defunct. At a journalistic level, Ignorance and Fantasy may feed simplistic or inaccurate narratives. Among citizens it may affect purchasing and shareholding/service user decisions and other civic participation
Examples (Healthcare)
(New examples are added to the top)
Our paperless Discharge Summary process generated about 5 times as many sheets of A4 as the old paper system, as the ‘paperless’ prescription got corrected and refined prior to discharge. Then we still were told we had to print a copy to go into the paper notes and of course the patient has to have a paper copy because there was no way to email it to the patient. The software could not message pharmacy, so we had to print out the discharge meds to be sent to pharmacy, who then checked found the errors, got doctors to correct them, then another print out, and round again. There are so many paper copies that sometimes an earlier incorrect paper copy gets filed into the notes. Then, unless someone hits ‘Finalise’, the pdf copy never gets emailed to the GP at all.
Dr Gordon Caldwell, Consultant Physician, @doctorcaldwell
Over the last few years there has been a call to enshrine ‘saying sorry’ in law. This became the ‘duty of candour’. When this was conceived it was imagined that people would find the guidance helpful and that it would make it easier for frontline staff to say sorry to patients when things have gone wrong. Patient advocates thought it would mean that patients would be more informed and more involved and that it would change the relationship from an adversarial to a partnership one. In practice this policy has created a highly bureaucratic process which has reinforced the blame culture that exists in the health service. Clinical staff are more fearful of what to say when something goes wrong and will often leave it to the official process or for someone from management to come and delivery the bad news in a clinical, dispassionate way. The simple art of talking to a patient, explaining what has happened and saying sorry has become a formalised, often written, complied duty. The relationships remain adversarial and patients do not feel any more informed or involved as before the duty came into play.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
“The higher up the national tree you go the more I would suggest that is the case. I feel there is an ever increasing disconnect again between what nationally is sometimes said to be going on and what people on the ground feel or see is going on. Politically, with a ’small p’, the message is put out that we are putting more money into the service than we ever did and it is the best health service around, but against that there is a frontline feeling that things have never been as bad as they are now and we can’t deal with the pressures.”
Sir Robert Francis QC, in an interview with Shaun Lintern for the Health Service Journal.
One of the procedures we carry out is a CT guided biopsy, where samples of tissues are obtained from a tumour inside an organ (usually a lung) using the CT scanner to guide us. On one occasion the equipment supplied for the procedure had subtly changed (though it was the same manufacturer), meaning that it was possible for the biopsy needle to sample 1cm deeper than expected. This was only discovered during the procedure.
Anonymous, Radiologist
The WHO Surgical Safety checklist was introduced into the National Health Service following the release of Patient Safety Alert Release 0861 from the National Patient Safety Agency on 29 January 2009. Organisations were expected to implement the recommendations by February 2010 including that ‘the checklist is completed for every patient undergoing a surgical procedure (including local anaesthesia)’. All organisations have implemented this Patient Safety Alert and the WHO Surgical Safety checklist is an integral part of the process for every patient undergoing a surgical procedure. Whilst the checklist appears to be used in every patient, there is clear evidence that there is variability in how the checklist is used both within an organisation and between organisations. Within an organisation, this variability can occur between teams with differences in the assumed value of using the checklist and within a team between individuals or professional groups. Its value can degrade to a token compliance process to ‘tick the box’. The assumption within an organisation at ‘the blunt end’ is that it is done on every patient.
Alastair Williamson, Consultant Anaesthetist, @TIVA_doc
Senior management often believe that all healthcare staff have received basic or intermediate life support training, as these staff work in the acute setting and would, of course, have received this training. In reality, life support competence is merely recommended and not mandated by bodies such as the Resuscitation Council (UK). This means that competence in life support is dependent on the number of resuscitation officers, whether staff have been released from work to go to training, etc.
Anonymous, Anaesthetist.
I think the simplest example of this is hand hygiene. Work-as-imagined (and indeed as prescribed) in this situation is that all healthcare staff follow the WHO Five Moments for hand hygiene. Multiple audits do of course reveal that our compliance (work-as-done) with hand hygiene is abysmal (especially amongst medical staff) with compliance rates of around 30%. Work-as-disclosed in regards to hand hygiene depends on who is asking – but again generally does not reflect work-as-done. Our patients however are mostly ignorant of our very poor levels of compliance in this regard.
Craig McIlhenny, Consultant Urological Surgeon, @CMcIlhenny
In 2005 my wife was admitted to hospital for a routine elective procedure. It took just over 20 minutes for people and a system that didn’t do human factors to leave my wife brain dead. It would be another 13 days before she really was dead. As clinicians the world over have reviewed my late wife’s case, in a quiet break room perhaps, they have all, with very few exceptions stated clearly: “I wouldn’t have done what they did”. Yet place those same people in a simulated scenario with the same real world disorder, which deteriorates into the same challenging moment, most actually do. This gap illustrates the difference between human performance as imagined and human performance in the real world. (Adapted from the Foreword of Human Factors and Ergonomics in Practice [CRC Press].)
Martin Bromiley OBE, Pilot and Chair of Clinical Human Factors Group, @MartinBromiley
There are high levels of burnout. A target-driven culture is exacerbating this problem. A typical example was when the government seemingly became convinced by poor quality data which suggested that dementia was under diagnosed So it decided to offer GPs £55 per new diagnosis of dementia. Targets were set for screening to take place – despite the UK National Screening Committee having said for years that screening for dementia was ineffective, causing misdiagnosis. And when better data on how many people had dementia was published – which revised the figures down – it was clear that the targets GPs were told to meet were highly error-prone. The cash carrot was accompanied with beating stick, with the results – naming and shaming supposedly poorly diagnosing practices – published online. Setting doctors harmful tasks, leading them almost to “process” patients, fails to respect patient or professional dignity, let alone the principle of “do no harm”. [Extract from article The answer to the NHS crisis is treating its staff better, New Statesman]
Margaret McCartney, General Practitioner, @mgtmccartney
This archetype is at the heart of the clinician-manager divide to the extent that it exists. (I understand that many clinicians get on well with many managers. And many wear both hats.) Senior managers (blunt end) may be ignorant of what clinicians (sharp end) do. They may have a fantastical view informed by preconceptions, unconscious bias, the views of intermediaries etc. The genesis of such a view may be consciously or unconsciously purposeful. Humankind cannot bear too much reality. It would be unfair not to say that in another sense clinicians (blunt end) may be just as ignorant of what senior managers do at their own equally sharp end. In the interest of the primary objective of the activities of both groups, high quality, safe patient care, a sympathetic mutual understanding is essential. No to ignorance. No to fantasy.
On the cusp of a major hospital change programme in 2009 I found myself at the centre of a situation that in the interest of patients required total cooperation between clinicians and managers. Unfortunately the way it was handled resulted in all out conflict.
On the one hand we had the board represented by the CEO. On the other the consultant body led by me. I had until recently been clinical director and understood the department, its workings and its history better than anyone. In between the two we had the three service managers, a midwife, an obstetrician and a recently arrived non-clinician who had not managed a clinical department before.
The CEO introduced a major change programme under the slogan “More for Less”. After this there was no direct contact with the consultants. The managers were her main conduit for the top down communication. The consultants were unable to stand fully together to either co-operate with positive changes or challenge initiatives which would jeopardise care. You may sense Reason’s cheese slices sliding into position here.
A RCPCH review later criticised senior management for the failed change programme being all about cuts and not service improvement, and for naively thinking that the soon to be commissioned PFI hospital would resolve deep relational issues (people are more important than buildings!). The middle managers were criticised for their aggressive managerial style. All nursing staff for example were put on notice of possible redundancy in a circular, without any face-to-face meeting. The wiser ones quickly jumped ship to adjacent Trusts. Two managers were accused of bullying by nursing staff, shouting, swearing, threatening job security etc. The consultants were unable to speak with a common voice. On the whole the clinicians had only one real interest – seeing patients. With the odd exception they were very good at that.
At this time I had become familiar with the ideas of Gerry Robinson, a management “guru” who had achieved a certain media profile. One of his central ideas on NHS management was expressed thus:
“I understand how this culture of multiple managers develops. I think Chief Executives get to a point where it is easier to manage other managers than it is to deal with medical and nursing staff, especially consultants, who can be resistant to being told what to do by those with no medical background. Instead, Chief Executives surround themselves with a safe set of managers who tell them what they want to hear, and perhaps they look to hire more – for business development or finance or new initiatives. Increasingly, the man or woman at the top of the tree is distanced from the reality of leading doctors, nurses and other staff, and delivering care to patients.”
I still believe there is a lot of truth in this. It is an arrangement that strengthens hierarchy and pits different groups against each other. (The remedy is fairly obvious by the way.) In our case we became locked in a triangle of mistrust. To different extents we all became the prisoners of our own fantastical views of each other with little or no desire to understand the other’s perspective. This fed the conditions that militate against co-operative working for high quality and safe patient care.
Older and wiser now I have at least come to understand in terms of organisational psychology why many of the actors in this tragedy behaved as they did. Where understanding falls short of a full explanation only agnosticism serves any purpose. A benevolent agnosticism.
I have one piece of evidence for the ignorant and fantastical view the CEO developed of me. The denouement was my own dismissal for, amongst other things, insubordination. Any CEO who views a senior consultant who has led his department for many years as a subordinate (as in some kind of military hierarchy) can only do so out of ignorance. It is essential that clinical/managerial teams are coalitions of equals who come to understand and respect each other. Only insecure leadership could believe otherwise.
In fairness to anyone I have criticised here there is nothing personal intended. In any case although I have put a fresh gloss on this the story has now been in the public domain for some years without those individuals making public comment.
David Drew, Consultant Paediatrician in a former life, @NHSwhistleblowr
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts