
This is the third in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence
- Taboo (this archetype)
- Ignorance and Fantasy
- Projection
- P.R. and Subterfuge
- Defunct
Each archetype includes a number of examples (currently healthcare-related). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 3: Taboo
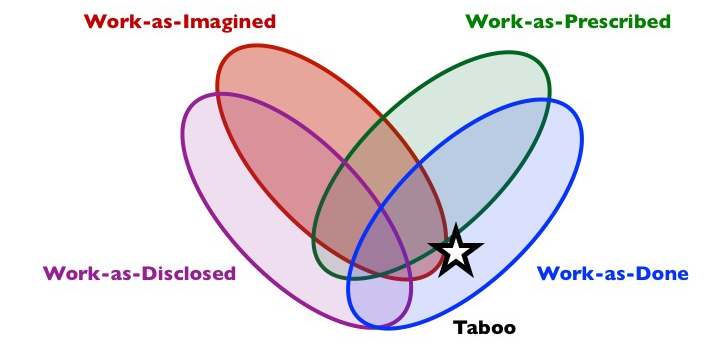
Composition: work-as-done but not as-disclosed, nor usually as-prescribed, nor usually as-imagined.
Short description: This is activity that people don’t want to talk about outside of one or more groups. It is often not in accordance with official policy, procedures, etc, or there is no relevant policy, procedures, or if it is described in procedures, others would find the activity unacceptable. As such, the activity is often not widely known outside of specific groups. The main defining feature is that it is not openly discussed.
What is it?
The Taboo archetype represents activity governed by social norms, but which is kept hidden, deliberately not disclosed outside of a defined group, usually for reasons associated with fear. The activity is often informal and not prescribed, but in some cases some prescription may exist but not be widely known. The activity will usually not be known outside of specific groups, though there may well be suspicion among others outside of these groups, though even this is still not widely disclosed. The distinguishing feature of Taboo is that disclosure of the activity is deliberately restricted, more so than will usually be the case with The Messy Reality, which is quite ordinary.
Those familiar with archetype are those who do the work, and those who sanction the practices (explicitly or implicitly), but it may concern work in any part of an organisation, from front-line to senior management. The Taboo archetype may exist in partnership with P.R. and Subterfuge, which may be used to throw out-group members off the scent of Taboo.
Why does it exist?
At the heart of Taboo is one or more conflicts between goals, needs, or values, concerning, cost, financial gain, efficiency, productivity, capacity, safety, security, satisfaction, comfort, sustainability, power, etc., and associated trade-offs and dilemmas. These conflicts may exist within and between groups.
The practices (work-as-done) that are pertinent to Taboo will usually be contrary to a prevailing norm (social, procedural, legal, moral or ethical) or expectation, such that if the activity were widely known, action may be taken that would be detrimental to the continuation of the activity. Hence, disclosure could be damaging to the goals, needs or values of the in-group.
Taboo may simply concern basic human needs, such as the need for rest or sleep, which are not catered for in the design or prescription of work. It is not unusual for sleep to be forbidden on nightshifts, and yet arrangements are made among staff to ensure that they get some sleep. In some cases, the practices might involve personal gain (e.g., remuneration, time off, power or prestige), perhaps associated with practices that might be seen as unfair or unethical, or that might trigger outrage if aired more widely. Taboo may also concern group-level needs (e.g., the need for survival or influence of an occupation). Often, the reasons for Taboo appear personal but are actually systemic, for instance involving perverse incentives, inadequate organisational processes, poor resources and conditions, inappropriate constraints, and goal conflicts. For instance, unhealthy and unsafe levels of overtime may offer financial benefits to individuals (pay) and organisations (fewer staff required), and thus may be form part of a Taboo archetype for both staff and management.
In many instances, there will be an efficiency-thoroughness trade-off (i.e., an emphasis on efficiency over thoroughness) or an acute-chronic trade-off in operation. Increases in demand and pressure, in an environment of inadequate resources, will tend to result in an emphasis on efficiency and short term goals, which will tend to breed practices which cannot be widely disclosed.
The Taboo archetype can, however, in conjunction with P.R. and Subterfuge offer groups protection from unhelpful or detrimental outside influence based on Ignorance and Fantasy of complex issues associated with work-as-done (e.g., safety margins or buffers, the need for resources). This is a complex issue that is difficult to understand without knowledge of the work.
Shadow side
What people can and can’t do and talk about openly sheds light on the shared assumptions, beliefs and values that underlie a group’s culture. Unsustainable, unethical or unacceptably risky practices can remain hidden, leading to ever wider gaps between work-as-imagined and work-as-done and potentially a drift into failure. Those who break the taboo (often referred to as ‘whistleblowers’) and disclose work-as-done may be outcast, from the group, organisation or profession.
Examples (Aviation)
(New examples are added to the top)
Flight Time Limitations: Regulatory Flight Time Limitations (FTL’s) that dictate pilot duty and rest times have changed, apparently to align with more recent research on fatigue. In reality, extremely fatiguing duty combinations can still be legally rostered. For 2-pilot long haul night flights it is not uncommon for pilots to lose 2-nights of sleep in 3 days. For 3-pilot flights where ‘horizontal’ rest used to extend allowable duty by half the rest period (e.g. 3 hours rest gives 1.5 hours credit) it now in many cases doubles it (i.e. 3 hours rest gives 6 hours credit). Fatigue is generally accepted by pilots as ‘part of the job’ are more inclined to cope than complain. The taboo subjects include the adaptive ways pilots are able to achieve rest (to remain safe) and the extent to which current FTL’s are a deliberate trade-off between safety and commercial interests. In the context of work-as-imagined, prescribed and done, the gap between them is very wide yet this appears to be accepted by all and regarded as necessary to satisfy different priorities.
Anonymous, Professional Pilot
Examples (Healthcare)
(New examples are added to the top)
A nurse at a children’s hospital shared the challenge of using BCMA (bar coded medication administration) technology during certain scenarios. The hospital pharmacy director implemented a system to track every time a nurses document administration but don’t scan the medication for any reason. If a nurse is found to do this repeatedly (again regardless of reason), they are “written up” and it negatively impacts future pay raises.
The nurse who shared the story related that often they had to use ointments (for instance, while caring for burn patients) that frequently got on the outside of the ointment container through normal handling. These ointments inevitably got on the bar code label making the medication impossible to scan.
The nurse then faced several options. They could try and obtain a duplicate bar code but this action was discouraged to prevent “work arounds” instead of scanning the medication to be administered. Second, they could administer the medication and not document it at all. Third, they could simply skip administration and avoid any issue.
Because of the administrative policy of the pharmacy, the nurse in question shared that she would on occasion skip medication administration or administer without documentation rather than risk punishment for a system-induced problem.
Matt Scanlon, Professor of Pediatrics, Critical Care, Medical College of Wisconsin
When working as a paediatric intensive care nurse we were often so busy that we had to figure out how we could do things in order to get through the shift with everything done. For example, in order to ensure the children received their medications on time we carried out a practice which was known to be poor. The nurse at the child’s bedside would draw up all the different medications (the children were often on at least 10 different types of infusions for intravenous route or oral medications, which were given in syringes via a tube connected to the child’s stomach). The nurse at the bedside would do the complicated calculations (the amount for the weight, concentration of the medication and route of administration). The nurse in charge of the unit would then go from bed to bed ‘assuming’ the nurse at the bed side had got it right and sign the prescription sheet to show that the medication had been ‘double checked’. This was not good practice, it was definitely not prescribed or imagined by the senior management and not discussed because everyone knew it was poor practice. As a result of this a number of errors could and did happen such as patients receiving the wrong dose (often as a result of a calculation error) or receiving the right drug but via the wrong route because of a mix up of the syringes.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
Organ preservation solutions are administered by registered practitioners during organ donation. These solutions are administered following death of the donor but are not formally prescribed by a doctor. Under any other circumstance, registered practitioners would not administer any fluids or drugs without a clear written prescription. Organ donation appears to be the only exception.
This is something that is not common knowledge outside the organ retrieval community. The main issue is that organ retrieval is a service commissioned by NHSBT, not directly provided by them so it is up to providers to enforce specific practices on the ground. However, this could create risks to individual practitioners if they were to administer organ preservation solutions incorrectly without prescription that resulted in harm to organs. NHSBT could potentially suffer reputational damage as an organisation and the practitioner (Nurse or ODP) would not be covered by the NMC/HPCC as are administering fluids without prescription and unlikely to be supported by their individual employing organisation for the same reasons.
The case of Dr Raj Mattu provides an example of Taboo. He was suspended by University Hospitals Coventry and Warwickshire NHS Trust in February 2002 on allegations of bullying, 5 months after he spoke to the BBC about the death of a patient in an over-crowded bay at Walsgrave Hospital, Coventry. A 5th bed was put into 4 bedded bay (so called ‘5 in 4’) in order that the hospital could never be deemed full. I worked as a Neurology SpR at the Walsgrave between January-December 2000 and it was the most stressful period of my career. I too was appalled at the policy of putting a 5th bed into 4 bedded bay (so called ‘5 in 4’) in order that the hospital could never be deemed full. Dr Mattu has faced years of mistreatment and ‘detriment’, and the effective end of his career at a cost for legal expenses alone of around £6 million. His successful employment tribunal was one of the most expensive in NHS history. However the most disturbing aspect of the Mattu case is that those responsible for the ‘5 in 4’ policy have faced no serious public scrutiny. How can we have any confidence that staff concerns such as Dr Mattu’s will be dealt with any differently the next time? The treatment of whistleblowers in the NHS is a reflection of the Taboo archetype: how whistleblowers are treated is often not openly discussed, nor prescribed, and hard to imagine.” (Based on a letter to The BMJ: http://www.bmj.com/content/348/bmj.g2881/rapid-responses.)
Dr David Nicholl, Consultant Neurologist, @djnicholl
When preparing intravenous injections for a patient, guidelines (e.g., NMC medicines management guidelines) and procedures require that the injection must be prepared immediately before it is due to be given, and not prepared in advance of this time. However, under current service pressures, including staff shortages and high acuity, doses may be prepared in advance to save time, or if prepared on time and then for some reason not given, may be stored to one side for later use, instead of being disposed of and re-made at a later time.
Anonymous, Pharmacist
Although most people would like to believe that admission to critical care does not depend on the bed status of the unit, this is not the case. If there are many critical care beds available, patients are likely to be admitted who would not be admitted if there was only one bed available.
Anonymous, Anaesthetist
Taboo describes the attitude of some healthcare workers to uniform policies. For example hospitals have a “bare below the elbow” uniform policy, where people can only wear a plain wedding band on the hands and forearms. Some people choose to ignore this and wear a watch, or a stoned ring. In theatre, this is most often ignored when people wear theatre gowns, as it is often cold in theatre, and no alternative is provided.
Anonymous
Nursing staff on night shifts take turns to have a 2-hour sleep if it is quiet. If it is busy then obviously it is all hands to the pump. This is not described in any job description but is tacitly known about and approved to ensure functioning if required.
Anonymous
With acute prescribing in GP practices, some medicines are kept separate from the repeat prescribing – generally quantities no longer than a month’s supply – with the general idea that these are meds that require a regular review by the GP to determine appropriateness of ongoing supply. Often, these are dealt with as “special requests”; the scripts are not run off by the admin staff with the regular repeat meds, but are passed to the GP (or they are run off by the admin staff but stored separately for the GP to review). The idea is that these meds have greater scrutiny and are not supplied in larger quantities, so there is a sort of a safety net around them becoming inappropriate long term medicines. The reality is these are often not given the greater scrutiny as intended and we see months of antidepressants and analgesics (to name a couple of drugs) issued every month with no proper patient review.
Anonymous, Pharmacist
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts