
This is the fifth in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence
- Taboo
- Ignorance and Fantasy
- Projection (this Archetype)
- P.R. and Subterfuge
- Defunct
Each archetype includes a number of examples (currently clinical). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 5: Projection
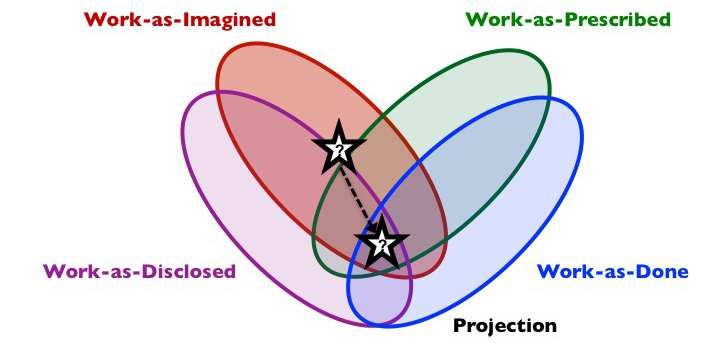
Composition: work-as-imagined, often as-prescribed and perhaps as-disclosed. May or may not be as-done.
Short description: We are prone to imagine that things will work according to a plan, and prone to wishful thinking, ignoring the potential for problems. The focus of Projection is the imagination of the future, as we think it will be, or would like it to be.
What is it?
When we need to design or plan human work, we project our imagination into the future. Informally, we plan our or others’ work, at some level, over the coming minutes, hours, days, months or years. Projection may involve planning a task about to be performed, via mental preparation, or the use of specific tools. Or it might involve planning a new system to be implemented some time in the future. This formal Projection might involve new or major changes to major infrastructure or facilities (such as hospitals, airports or railways), changes to equipment, changes to staffing and competency, changes to artefacts of management (such as performance targets or league tables) or changes to procedures. For changes to the design of work, there will be some kind of prescription of how we think things should happen, and this may be communicated to others, in designs, plans, procedures, etc. We might also try to project what we don’t want to happen, perhaps via hazard identification or risk assessment.
Why does it exist?
Projection serves our need to reduce fear and uncertainty about the future, and have some confidence that our future needs will be met.
Shadow side
In our attempts to bring future work-as-done into the present, Projection will often be far from the mark, and will usually be inaccurate in some way or other. Even when you are familiar with work-as-done now, Projection of future work-as-done, and related resources (including time), can be very unreliable. We tend to overestimate the degree to which future work-as-done will follow our designs and plans (due to overconfidence, lack of imagination, wishful thinking, variability in demand and resources, etc.). We also tend not to foresee unwanted side-effects or long-term consequences of our designs and plans. Even small changes can have disproportionately large effects/
It is difficult to project with accuracy even seemingly straightforward activities, but as work becomes more complex, emergence becomes the thorn in the side of Projection. We try to overcome this with the application of formal methods, but most of these involve decomposing future tasks and related systems into parts, considering these parts, and using these parts to project performance. Because of interactions between activities and the environment, adaptation, and the effects of multiple changes over time, future work-as-done cannot always be projected in this way, and so is often not as expected. The mismatch between what we expect and what happens will tend to increase with complexity.
At the blunt end, those involved in the design of future work may engage in Projection on a basis of Ignorance and Fantasy, especially if they are distanced from The Messy Reality of work-as-done even today. Close proximity to work-as-done is no guarantee of success in predicting the future, but increasing distance – which is common – stretches the feedback loop back to imagination and design.
As work-as-done comes into fruition, other archetypes emerge. The Messy Reality will tend to rise to the surface, of course alternating with Congruence, and instances of Taboo may also emerge as certain aspects of work – at the blunt end or sharp end – cannot be discussed openly, perhaps replaced with P.R. and Subterfuge. Unwanted effects are covered up by day-to-day adaptations at the sharp end, perpetuating Ignorance and Fantasy at the blunt end. The Defunct archetype will also tend to unfold over time, as policies, procedures and plans remain docked in the work-as-imagined of days gone by…
Examples (Healthcare)
(New examples are added to the top)
When we created the list of ‘never events’ at the National Patient Safety Agency we genuinely thought that it would lead to organisations focusing on a few things and doing those well. We thought it was a really neat driver for implementation of evidence based practice (e.g. the surgical safety checklist). We ignored the potential for using never events as a stick to beat people up with, we ignored the potential for gaming the data, we ignored the potential for people to become fearful of reporting and the loss of learning as a result. We importantly ignored the fact that in the vast majority of cases things can never be never – that it is a fact of life that things can and do go wrong no matter how much you try to prevent it. There is no such thing as zero harm and the never events initiative unfortunately gave the impression that it could exist.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
The computerised estimation of the time it will take to perform a case in theatre can be an example of Projection. Theatre scheduling uses the average time that similar cases have taken in the past to predict how long a case will take in the future. Individual patient, surgical and anaesthetic factors are not considered. Sometimes this is accurate, but other times it is not. It is therefore a crude system, although it is the best that we have at present. The problem comes when staff feel they have failed when cases take longer than the projection and theatre over runs. This is inevitable given the nature of the system.
Emma Plunkett, Anaesthetist, @emmaplunkett
Installation of computerised medical systems can display this trait. For instance with the installation of a fully computerised system for ordering all sorts of tests (radiology requests, lab requests, etc.) work-as-imagined (and -as prescribed) was that this would make work more efficient and safer, with less chance of results going missing or being delayed. Prior to the installation there was much chat (work-as-disclosed) with widespread talk of how effective and efficient this would be. After installation it became apparent that the system did not fulfill the design brief and while it could order tests it could not collate and distribute the results. So work-as-done then reverted back to the system that was in place before where secretaries still had to print results on bits of paper and hand them to consultants to action.
Craig McIlhenny, Consultant Urological Surgeon, @CMcIlhenny
There are a lot of discussions about how electronic solutions will solve all the problems! Medicines reconciliation still remains a challenge, on admission and discharge, and there is great faith put into how electronic solutions will solve these. They are seen as reducing risks but often just introduce other different risks. Fundamentally we still need competent practitioners to be able to use good clinical judgement and clear decision making for them to be effective.
Anonymous, Pharmacist
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts