
One way to understand the links between unwanted events, conditions and interventions is via causal loop diagrams. These represent how situations perpetuate in ‘causal loops’. They are depicted as words and phrases for events and conditions, and arrows with a plus or minus sign to indicate the direction of causal influence. Causal loop diagrams can assist a conversation via the gradual building of each loop. They can otherwise represent data from research and practice.
In this post, I illustrate the progressive build of a causal loop diagram concerning reactions to unwanted events, including fixes that fail, based on practice and research. This might be useful to professionals seeking to understand why unwanted events continue to occur despite, or because of, interventions. The diagram is not ‘complete’ and would be drawn differently for different purposes, contexts and situations.
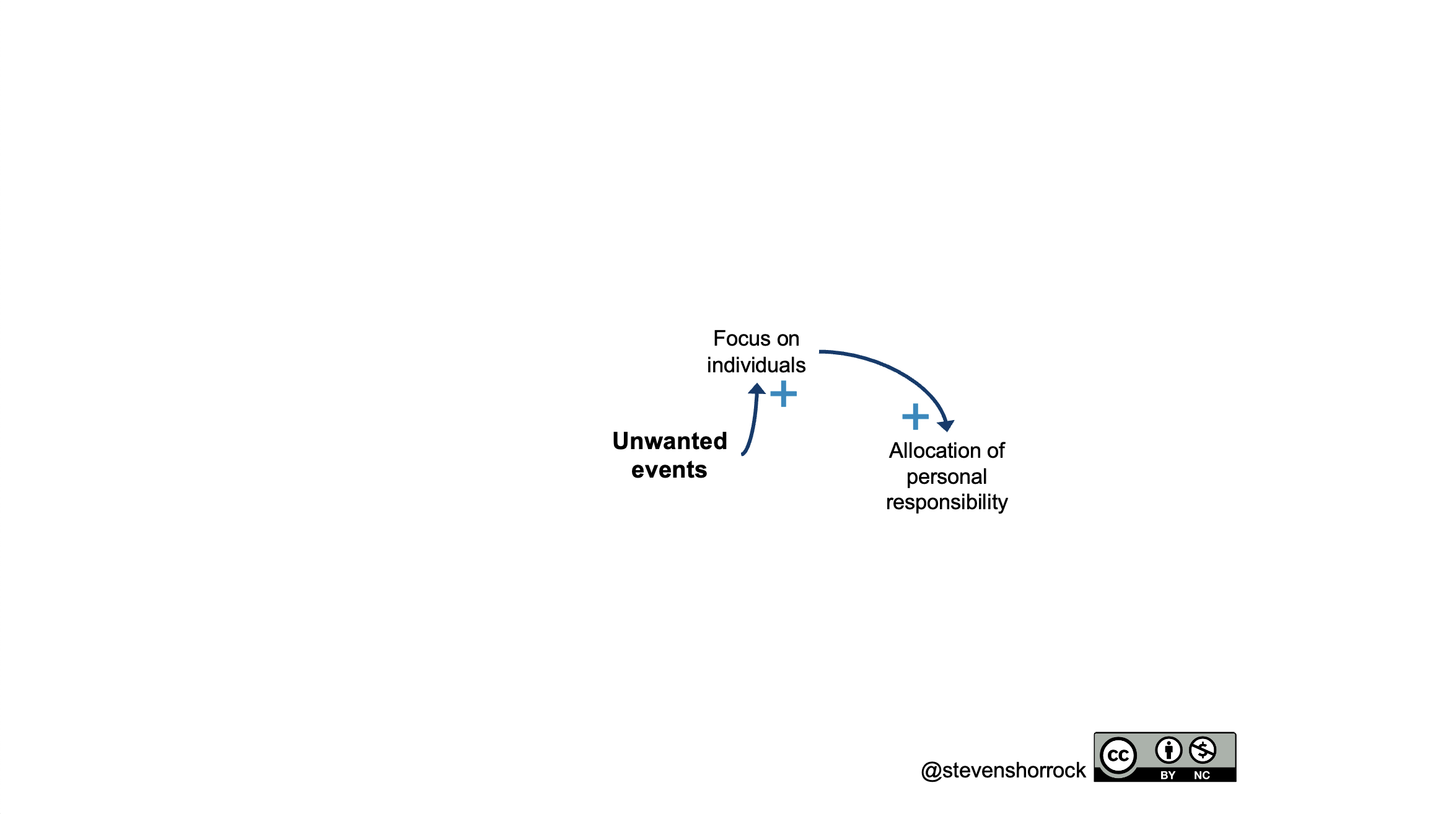
Focus on individuals
What we often see after unwanted events is a focus on individuals. Part of this may be what I refer to as an inappropriate simple-to-complex attribution error. This can affect us all. It is where our responses to an unwanted event in relatively simple situations (e.g., someone spills their drink onto you) is transferred to situations where the specific behaviour seems simple but the situation and broader context is complex and hard to see. Examples can be found in many major accidents where a front line operator did something that they were not supposed to do, or did not do something that they should have done…in hindsight. There are many examples, such as the train crash in Santiago de Compostela in 2013 and the mid-air collision over Uberlingen in 2002. The focus on individuals and their errors is a ‘first story’ perspective, characterised by high personalisation, low complexity, and low context. While the errors of front line professionals take a central role, those at the blunt end are fuzzy and become ‘context’, and yet create invisible tripwires and trapdoors for anything but perfect performance in the seconds and minutes of operations. All of this naturally leads to allocation of personal responsibility to the person at the sharp end of operations. We see this in the start of the diagram below.
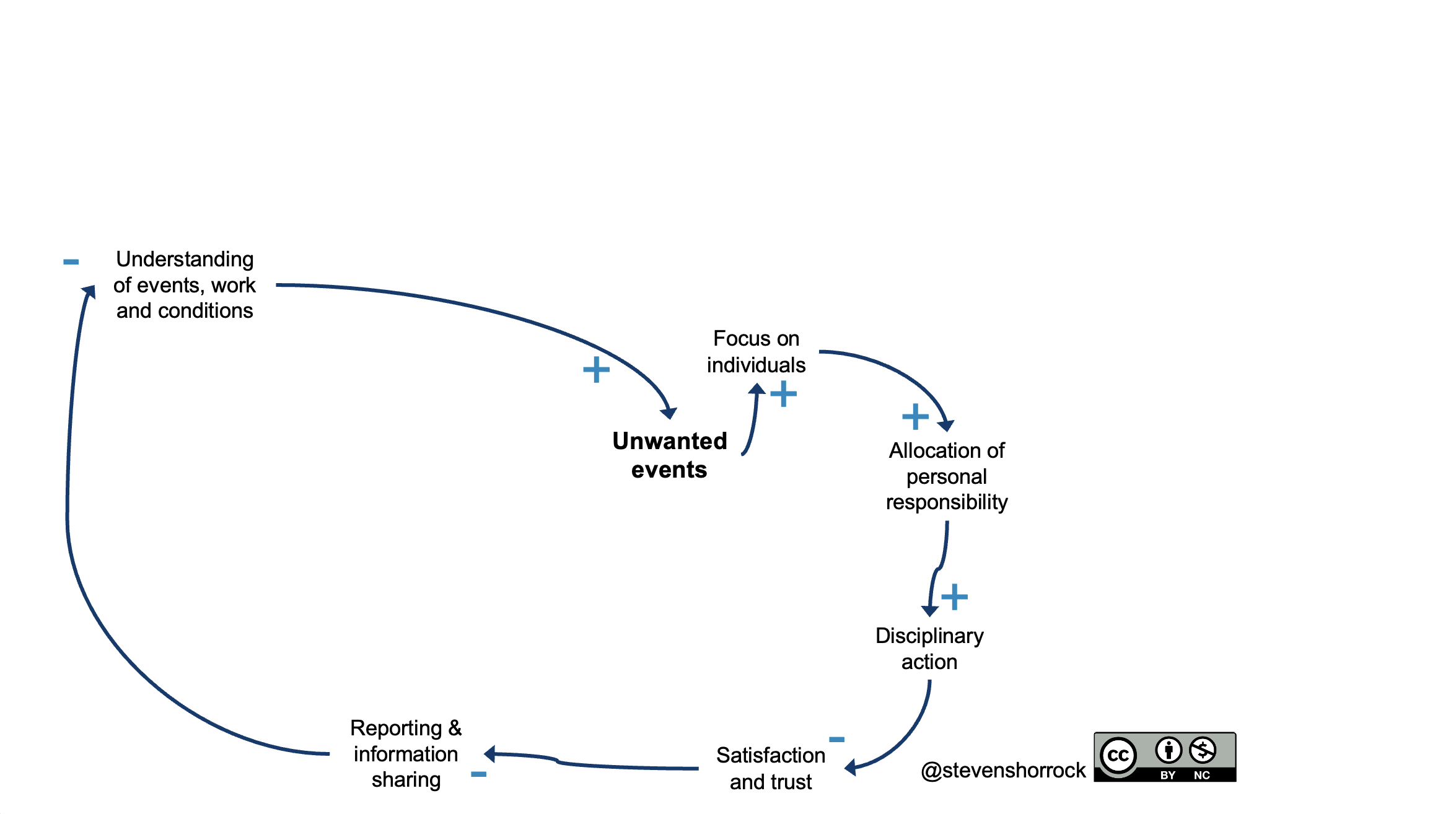
Disciplinary Action
With more responsibility allocated to individuals at the sharp end of operations, it may seem natural, just and logical for disciplinary action to follow, and so we often see a reinforcing relationship – more allocation of personal responsibility, more disciplinary action. This is more common in some national, organisational, and professional cultures than others. But with more disciplinary actions comes less satisfaction among staff and less trust in management, especially in terms of what will happen if staff report (or are involved in) unwanted events. Lower satisfaction and trust is associated with reduced reporting and information sharing, since there is a fear of disciplinary action. With less reporting and information sharing comes reduced understanding of events, work and conditions in the organisation, which in turn is associated with more unwanted events. This completes a causal loop.
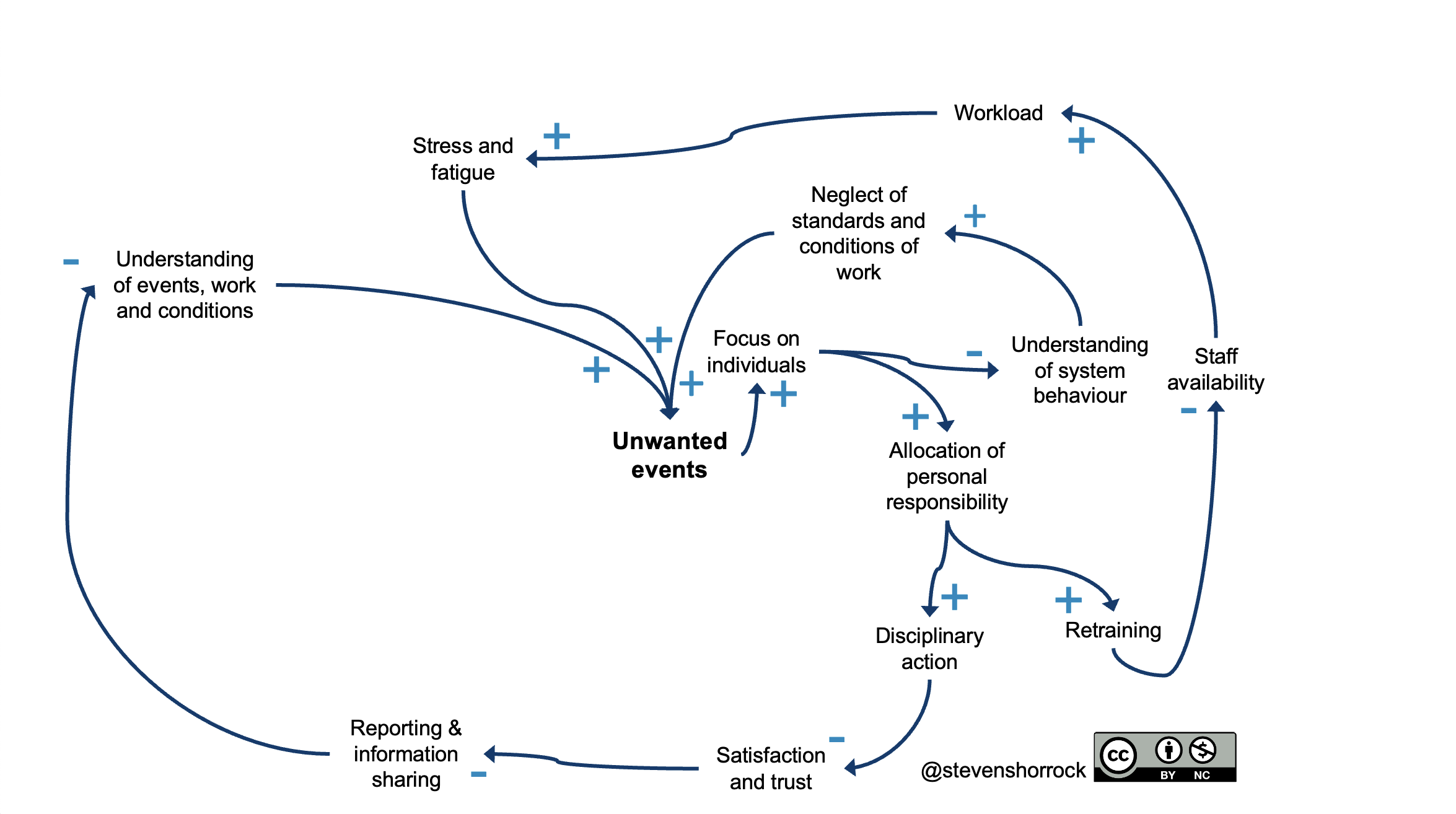
Retraining
Now we go back to allocation of personal responsibility. This is often associated with retraining as another intervention. Again, this may seem logical: if individuals are held to be responsible for unwanted events, then there must be a competency problem, which requires retraining. Unfortunately, retraining individuals has a number of side effects. One of these is removing the person from the available workforce for a period, resulting in higher workload for those staff who are available. This can be associated with more stress and fatigue, which can contribute to unwanted events.

Understanding of system behaviour
A focus on individuals (a foe of intervention) is also associated with reduced understanding of system behaviour – the complex patterns of interaction, adaptation and self organisation. The paucity of understanding is associated with a neglect of standards and conditions of work. Practically, this may mean: a practical drift resulting in a widening gap between work-as-prescribed (and work-as-imagined) and work-as-done; degraded maintenance or a lack of spare parts, with reduced reliability or redundancy; inadequate staffing; deteriorating facilities; poor services for staff; lack of training opportunities; etc. The focus on individuals has left the organisation exposed to degradation. Again, we see expression in unwanted events.
Reactive introduction of new and changed procedures
We now come to a new reaction to unwanted events: reactive introduction of new and changed procedures. This is an alternative to a focus on individuals, though both may occur simultaneously, albeit illogically. Changing a procedure may make sense, but when done reactively and with haste (another foe of intervention), there is more chance of unintended consequences, as in this example. One of the implications can be increased complexity. New or changed procedures may have more steps or conditions, or may conflict with other procedures (this cross-check is often neglected). It also seems to be far easier to introduce procedures than remove defunct procedures, bringing new forms of jeopardy to staff. At a certain level or pace, increasing complexity tends to be associated with reduced quality of human performance, since staff have to make sense of their worlds and respond appropriately, while unable to understand fully the potential implications of their interventions. And reduced quality of human performance, not surprisingly, tends to be associated with unwanted events.

Regulatory and media attention
At a certain degree of severity or frequency, unwanted events are likely to attract regulatory and even media attention. This is normal, and so is to be expected. In the organisation, it is also normal that regulatory and media attention will attract management attention. Something must be done. In the urge for urgency, any change is better than none, and reactive introduction of new and changed procedures may seem like a good option. This demonstrates that something has been done, though the change may demonstrate work-as-imagined solutioneering. Alternatively, there may be focus on individuals and even scapegoating (again, a foe of intervention). This is especially likely when an unwanted event is woven into a ‘human-error-as-cause’ narrative (a foe of explanation in system safety), which often makes an appealing headline. Both of these approaches lead into loops already described, increasing the likelihood of further unwanted events.

Notes on causal loop diagrams
Causal loop diagrams focus on situations and are used to model causal interconnections within a (typically problematic) situation. They attempt to model actual causal interconnections or interrelationships among variables within a situation, expressed as words or phrases. They are not ‘complete’ depictions of a situation, but should be as complete as necessary for the purpose of the analysis. Causal loop diagrams are normally drawn without predefined structure or levels (e.g., as can be found in AcciMaps, in a causal sense), such as society, industry, organisation, team, and individual. There are alternative labelling conventions for errors (e.g., see Open University guidance here). Different software packages can be used, but sticky-notes often remain the most useful development method for in situ groups.
Concluding thoughts
Causal loop diagrams may help to understand a situation, get new perspectives and reveal blindspots, determine points of leverage for intervention, and explore options for intervention. It is then possible to explore the likelihood of success of the options for intervention and the level of commitment to these. It’s important to remember that diagrams can be drawn in all sorts of different ways. The key thing is the conversations, questions and insights that arise in the process of creation.
Related Posts
https://humanisticsystems.com/tag/ep8/
https://humanisticsystems.com/tag/just-culture/
https://humanisticsystems.com/tag/systems-thinking/
How to cite (APA)
Shorrock, S. (2024, January 29). “Why Are We Having More Incidents?” Causal Loops in Reactions to Unwanted Events. Humanistic Systems. https://humanisticsystems.com/2024/01/29/why-are-we-having-more-incidents-causal-loops-in-reactions-to-unwanted-events/
Creative Commons Licence
“Why Are We Having More Incidents?” Causal Loops in Reactions to Unwanted Events © 2024 by Steven Shorrock is licensed under CC BY-NC 4.0
This license requires that reusers give credit to the creator. It allows reusers to distribute, remix, adapt, and build upon the material in any medium or format, for noncommercial purposes only.
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

That was beautifully explained, thank you Dr.!
Re-reading the diagram, it was clear what the differents flows of the loop all ended in more incidents, but what else the flows generate? I Mean, what else good ? There is some things in the loop that can actually prevents another types of incidents… for instance: “Retraining” in the flow causes less staff availability but also causes more understanding of system behavior.
I Think that should count too.
LikeLike
Yes, that could be another loop if it were a valid measure, but in this case the focus on the person and retraining is futile because it won’t prevent incidents. There is no link here between retraining (eg of operational procedures) and understanding of system behaviour.
LikeLike