
This is the seventh and last in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence
- Taboo
- Ignorance and Fantasy
- Projection
- P.R. and Subterfuge
- Defunct (this Archetype)
Each archetype includes a number of examples (currently healthcare-related). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 7: Defunct
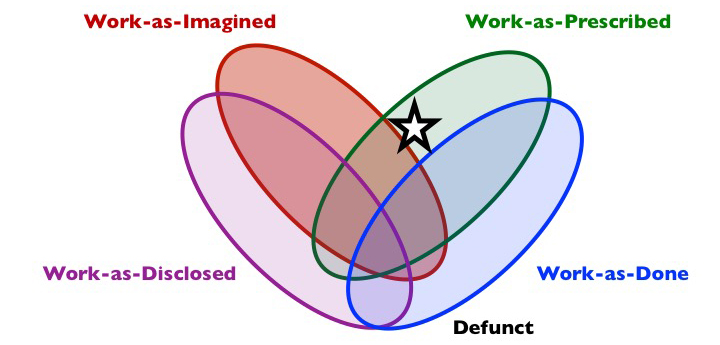
Composition: work-as-prescribed but not as-done. May or may not be as-imagined or as-disclosed.
Short description: Some forms of prescribed work are not enacted, or else drift into disuse, but are still officially in place. Some will imagine that these are in place, while others know or think they are not. However, the existence of the Defunct work may be used to judge actual activity.
What is it?
Much human work exists in prescribed form, such as regulations, management systems, policies, procedures, guidelines, checklists, good practice, user interface dialogues, etc. Sometimes, this work-as-prescribed does not reflect the reality of work-as-done, which might be characterised as The Messy Reality. The prescribed work still exists, but in a form which is Defunct. Sometimes, this is just a temporary matter, where work-as-prescribed for some reason does not apply. Other times, work-as-prescribed may be permanently Defunct. Work-as-prescribed may even seem quite irrelevant; few would even think about it or discuss it, let alone follow it, especially at the front line of work, or even throughout an organisation or industry sector.
Why does it exist?
It is often the case that Defunct designed work has been prescribed without adequate attention to the design process, often an efficiency-thoroughness trade-off at the blunt end. A thorough approach to design (of interfaces, procedures, checklists, etc) would require that: 1) the stakeholders (especially the users), system, activities and context are understood; 2) stakeholder needs are investigated and design requirements specified; 3) prototypes are developed; and then 4) prototypes are tested. The testing would reveal any flaws in the implementation of this process, and thus there would be iterative loops back to each stage. If the prototype (e.g., checklist) meets the users’ and other stakeholders’ needs, then we have a final step: 5) implementation. The whole process would be planned with appropriate resources allocated (expertise, time, etc). This is a thorough approach, known as human-centred design (or ergonomics).
The ‘efficient’ approach, which is more common, is to go straight to step 5 (implementation), perhaps with some perfunctory consideration of step 1. Commercial-off-the-shelf/pre-designed systems and artefacts are often purchased, which is understandable and often completely necessary. The problem is, neither the developer nor the purchaser may have completed the previous 4 steps. Even if the developer has used some kind of human-centred design process, the new context and stakeholders (and therefore the stakeholders’ and users’ needs and design requirements) may well be very different. Since there is no testing, feedback is gathered in real operations, by which time it is too late. Local adaptation of the artifact (e.g., checklist, user interface dialogue) to the users’ needs may be impossible, prohibitively expensive or impractical.
People at the sharp end are now faced with a Catch-22. Either they comply with work-as-prescribed (Congruence) or they find another unprescribed solution (The Messy Reality) and the work-as-prescribed is Defunct. In either case, work-as-done may have unintended and unforeseen consequences.
Even with human-centred design, work-as-prescribed may fall into disuse. Such cases are often a mystery to those at the blunt end and even many at the sharp end. This tends to happen when the work-as-prescribed is not understood, either the details or the purpose. In such cases, continuous monitoring and discussion of work-as-done is likely to be helpful, with appropriate adjustment and education where necessary.
There may also be cases where work-as-prescribed is simply not annulled or abolished when it should be. Many organisations and governments have numerious policies, procedures, regulations, laws and so on that remain officially in place, but that no-one imagines are in use. (British law is replete with such laws. For instance, Section 54 of the Metropolitan Police Act 1839 makes it an offence to carry a plank of wood on a pavement.)
Shadow side
Many of the problems associated with the Defunct archetype concern the nature of work-as-done and work-as-imagined, and so are associated with other archetypes, especially The Messy Reality and Ignorance and Fantasy.
In some cases, work-as-prescribed is Defunct only in particular circumstances. This was the case with the QF32 engine failure. The Airbus A380 ECAM checklists could not be followed as prescribed. In such cases, the people in control are deep into The Messy Reality and have to use their judgement and experience to find alternative solutions to the problems that they face. If appropriate training is not provided to help deal with such exceptional events, then the assumption that work-as-prescribed is universally safe becomes a particular liability.
In other cases, work-as-prescribed is more or less permanently Defunct. This presents some different problems, again mostly associated with other archetypes. A particular problem concerns the consequences of not working to rule. Gaps between work-as-prescribed and work-as-done may be the basis for disciplinary and regulatory/legal action against individuals and organisations. In some cases, such action may be unfair and vindictive, for instance when Defunct rules are used for used as a tool for workplace bullying.
Finally, an obvious problem with this archetype is that the Defunct work might actually represent good practice with benefits for safety, health, or other goals. In this case we need to try to understand why the work-as-prescribed failed to make it over the line of reality.
Examples (Healthcare)
(New examples are added to the top)
Aircraft Type changes: When an airline introduces a new aircraft type, ‘defunct’ procedures from existing aircraft types can remain in the system whilst new operational procedures take their time to bed in. During this time, pilots may purposefully deviate from existing procedures on the grounds of ‘airmanship’ if they consider it to be in the greater interests of safety. However, the pressure to comply with SOP’s can blur the lines and compromise safety when defunct procedures are blindly followed.
For example, the operational and performance implications of an engine fire on take-off are very different between 4 and 2 engine aircraft. In the 2-engine case it is paramount to check the status of both engines before you shut one down as there are situations where you could inadvertently leave yourself with no engines. This is less critical on 4 engine aircraft as you will still have 2 or 3 engines left, so the procedures vary to reflect the different priorities.
When my airline introduced 2 engine aircraft it retained its 4 engine procedures for engine failures on take-off for over a year. During this time we were expected to comply with the old (defunct) procedures for check purposes, that few would have followed for real. I recall being reprimanded in a simulator check for restarting a failed engine on take-off, yet by my next check I would have been reprimanded for not doing it. Ultimately the uncertainty caused a real-time operational safety event, after which 2 engine procedures were quickly implemented.
Anonymous, Professional Pilot
Examples (Healthcare)
(New examples are added to the top)
Most NHS organisations have policy in place restricting staff working on the operating theatres from wearing their scrubs outside the theatre department. However, staff are aware that their scrubs are uniform, not personal protection equipment, and therefore do not adhere to this policy, on the most part. The organisation does not enforce this policy either. Although this policy is effectively defunct, staff can still be judged and potentially punished for non-adherence.
Most healthcare policies are defunct! They are too long and so somewhere in the depths of the documents there will be things that are no longer applicable. They are usually written once and then updated yearly (often the yearly review is delayed or forgotten) so they get out of date quickly. Healthcare (and clinical care in particular) is constantly updating with new knowledge or changes to the organisation which is rarely reflected or delayed in its reflection in a policy or procedural document.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
The UK GMC clearly states that all medical notes should clearly and legibly document who has made a decision, who is documenting the decision and when the decision was made. This is widely published by the GMC in ‘Good Medical Practice’ and all healthcare professionals are aware of this.
Despite this guidance it is known and repeatedly demonstrated in medical literature that this is not the case. This is a danger to patient safety and a contributor to system failure.
Hospital policies repeatedly include this guidance despite it being well understood that it is commonly not achieved.
Anonymous
Of the 2184 policies, procedures and guidelines (PPGs) in my organisation, 28% are currently out of date and may therefore not reflect current practice. More interesting still, are the nearly 19% of PPGs that have been opened less than 5 times in total, including by their authors. These documents are often written to meet the requirements of external agencies with the idea that not having a policy leaves the organisation vulnerable to criticism. These documents remain unopened, unused and unrelated to daily work but may be used after incidents as a form of organisational protection: “yes, we had a policy for that”.
Carl Horsley, Intensivist, @horsleycarl
In operating theatres that use lasers, certain precautions, rules and safety precautions have to be in place. Part of this is to have a risk assessment and standard written laser protection policy. This risk assessment is normally carried out by a laser protection supervisor from a distant site who has no knowledge of local practice. In addition this tends to be written when a new laser is purchased and then is never updated. While work-as-imagined would be following the policy to the letter, if the policy is impractical for the local use of the laser, the local team will tend to develop workarounds (The Messy Reality). When there is a site visit by the laser protection supervisor however, work-as-disclosed will follow work-as-imagined – as they are reassured that everyone follows all the rules to the letter (P.R. and Subterfuge). If a laser protection incident does however occur, the local team would all be held to account by the Defunct laser protection rules.
Craig McIlhenny, Consultant Urological Surgeon, @CMcIlhenny
When the surgical team book a patient for theatre, they are supposed to discuss this with the anaesthetic team, to explain the indication for surgery, the degree of urgency and any medical conditions the patient has. The anaesthetic team should therefore be a central point who are aware of all the patients waiting for theatre to help with appropriate prioritisation. In reality this only happens if they happen to see an anaesthetist when they book the case. More often than not, cases are “booked” with no discussion with the anaesthetist and often the cases are not ready for theatre (may need scans first for example) or may not even need an operation. This only becomes obvious when the anaesthetist goes to review the patient, or perhaps even later. Despite many organisations having guidelines about this, it still seems to happen.
Emma Plunkett, Anaesthetist, @emmaplunkett
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts