
This is the sixth in a series of posts on The Archetypes of Human Work, which are based on the interactions or relationships between The Varieties of Human Work. For an introduction, see here.
The seven archetypes are:
- The Messy Reality
- Congruence
- Taboo
- Ignorance and Fantasy
- Projection
- P.R. and Subterfuge (this Archetype)
- Defunct
Each archetype includes a number of examples (currently healthcare-related). If you have further examples – from any industry – please provide an example as a comment or get in touch. More examples will be added over time.
Archetype 6: P.R. and Subterfuge
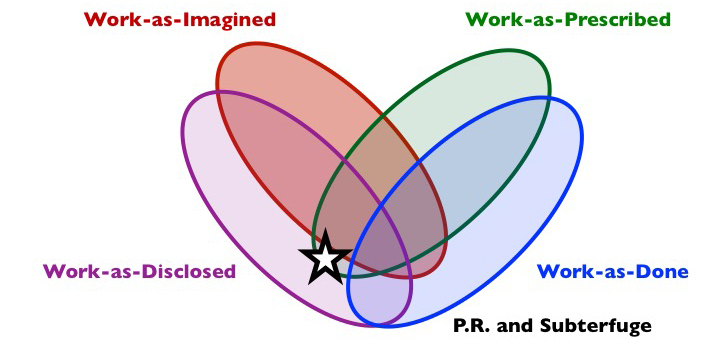
Composition: work-as-disclosed and often as-described but not as-done. May or may not be as-imagined by the discloser.
Short description: This is what people say happens or has happened, when this does not reflect the reality of what happens or happened. What is disclosed will often relate to what ‘should’ happen according to policies, procedures, standards, guidelines, or expected norms, or else will shift blame for problems elsewhere. What is disclosed may be based on deliberate deceit (by commission or omission), or on Ignorance and Fantasy, or something in between… The focus of P.R. and Subterfuge is therefore on disclosure, to influence what others think.
What is it?
Work-as-disclosed is what people say (in verbal or written form) about work-as-done by themselves or others, and is the dominant variety of human work in the P.R. and Subterfuge archetype. ‘P.R.’, in this context, could stand for ‘Public Relations’ or’Press Release’, which focus on disclosure but not necessarily reality. P.R. could also mean ‘Pre-Reality’ (disclosing that something is real before it really is real) or ‘Post-Reality’ (where “words don’t matter nearly as much as the intent, the emotion, the subtext…”, Seth’s Blog). It might also be seen as what is now called ‘alternative facts’ and fake news. P.R. and Subterfuge is commonly associated with politicians, spin doctors, lawyers, lobbyists, reporters, public relations specialists, sales people, and advertisers, but will be familiar to most, to some degree.
P.R. and Subterfuge tends to concern what in-group members say about work-as-done to out-group members. It is especially evident when people have to disclose the circumstances of failures or compliance with regulations, management systems, policies, procedures, guidelines, checklists, good practice, etc. to internal specialists (e.g., auditors, investigators, competency assessors, doctors, HR, senior managers) or outside agencies, organisations or individuals (e.g., regulators, supervisory bodies, professional associations, judiciary, journalists, citizens, interfacing organisations). It includes what is said or written, and what is not, in audits, investigations, inquiries, press releases, interviews, freedom of information requests, corporate communications, social media, etc.
P.R. and Subterfuge may involve varying levels of deception. Generally, where the consequences of disclosure are pertinent, unless the other party is trusted, people will tend to describe the work that they do in a way that accords with work-as-prescribed or (what is thought to be) work-as-imagined by other party. In some cases, the difference between work-as-disclosed and work-as-done with P.R. and Subterfuge is very much deliberate, from minor omission to large scale cover-ups. In such cases, a partner archetype will often to be found in Taboo; the aspects of work-as-done that cannot be discussed openly will be omitted from P.R. and Subterfuge. In other cases, there may not no intentional deceit on behalf of the discloser, but what is disclosed may be fed by subterfuge by others.
Why does it exist?
There is often a need to describe or explain performance, both internally within organisations and outside of organisations. What is said (work-as-disclosed) will clearly influence the work-as-imagined of these others, and this is the primary purpose of P.R. and Subterfuge. Because work-as-disclosed does not align with work-as-done, P.R. and Subterfuge will tend to feed the archetype Ignorance and Fantasyin others, inadvertently or deliberately.
The reasons for P.R. and Subterfuge are varied but many of these can be grouped into two major categories: ignorance and fear. Often, those who are distant from work-as-done talk about it based on Ignorance and Fantasy. Such individuals are reliant on their work-as-imagined, knowledge of work-as-prescribed, and work-as-disclosed by others. For instance, a corporate communications specialist, press officer, or a senior manager, will tend to know little about the specifics of how front-line workers actually work, and will rely on others for this information.
P.R. and Subterfuge can also be motivated by fear of possible consequences should the reality of work-as-done be revealed. These consequences for individuals and organisations may relate to legal action, bad publicity, journalistic inquiry, regulatory investigation or sanctions, fines, cut backs to funding or resources (e.g., staff, training), loss of reputation or status (individual or organisational), loss of profession, operating/professional licence or livelihood, and in extreme cases, loss of liberty. The perceived risk of such consequences will tend to shape what is disclosed, what is not, and what else is said.
It may seem like P.R. and Subterfuge is the product of dishonest organisations and individuals, but a number of systemic features of organisations and industries can cultivate the archetype. Examples include aspects of regulatory practice, management control measures, procedural constraints, measures, information flows, performance targets, incentive systems, punishments, and goals (especially goal conflicts). In the face of conditions or interventions that get in the way of the work (and potentially make it unsafe or otherwise ineffective), individuals and groups may justify P.R. and Subterfuge via a perceived higher purpose or goal. An illusion of Congruence may be created for out-groups, perhaps in response to the Defunct archetype, or to try to see off damaging interventions based on a superficial and inaccurate perception of work-as-done, such as cutbacks to resources (e.g., cutbacks to staff based on observation of a quiet period) or inappropriate constraints (e.g., procedural diktats based on one incident). P.R. and Subterfuge may therefore offer perceived benefits by protecting people from unwanted and potentially damaging outside influence or intervention which does not recognise the reality of work.
Shadow side
P.R.and Subterfuge, especially in its more deceptive form, involves a variety of ethical problems and dilemmas. More generally, it increases further the distance between work-as-imagined and work-as-done. Work-as-prescribed may become increasingly detached from reality, perhaps Defunct, thus invalidating many organisational and regulatory control measures, which are tied to work-as-prescribed. Work-as-done (and associated risks) remains unknown to most stakeholder groups. This creates problems of safety, accountability and liability.
In many industries, organisations have been known to cover up work-as-done (especially The Messy Reality) when things have gone wrong (see this reported decades-long cover-up by Dupont, which has long promoted itself as a “world class safety leader”). In explaining failure, the activity of an organisation may be Taboo, and what is disclosed may differ markedly from what is found by an independent inquiry. In 2016, four Dupont workers died in a toxic gas leak four workers died in a toxic gas leak (see here). The U.S. Chemical Safety Board inspectors said the reasons for the accident related to the corporate safety culture nationwide, citing design flaws in DuPont’s complex pesticide production unit, inadequate gas detectors, outdated alarms and broken ventilation fans. DuPont, the company originating from the founder of the ‘zero injury’ philosophy (chemist and industrialist Éleuthère Irénée du Pont de Nemours, 1771-1834), attributed the cause of the disaster to actions by rank-and-file employees. The tendency of organisations to point the finger at sharp end workers is an example of P.R. and Subterfuge which perpetuates P.R. and Subterfuge among rank-and-file employees, in order to protect themselves from blame; a spiral of subterfuge.
Examples (Aviation)
(New examples are added to the top)
Annual refresher training for Safety and Emergency Procedures: The time pressure to ‘tick the legal boxes’ in over-crowded curricula is immense. Learning is frequently compromised for compliance as training gets dampened down to absolute minimum requirements. This can lead to some interesting workarounds to create the false impression that work as prescribed is complete.
On one occasion during my annual refresher training for SEP (Safety and Emergency Procedures) an instructor carried a fire extinguisher around the group. We all reached out and ‘touched it’, thereby satisfying the regulatory requirement to ‘handle’ a fire extinguisher.
On another occasion a ‘legally required’ document was read out to us (a group of 40) in its entirety at high speed. The group started giggling after page one (of three) as no one could take it in. At this point we were all told off for not listening and reminded of our legal responsibility to “know this stuff”. No handouts or summaries were offered. Those of us who challenged the teaching approach after the session and got defensive replies. Afterwards over coffee few could even recall what the document was about, though I assume to this day I remain legally ‘qualified’ to handle the content it contained.
Anonymous, Professional Pilot
Examples (Healthcare)
(New examples are added to the top)
I have interviewed many people during incident investigations who have said what they thought I wanted to hear – what the guidance says or what the policy says rather than what actually happened. This is for many reasons, some may even have convinced themselves that it did, some will be lying, some will be fearful of getting themselves or others into trouble so they may not lie but may not tell the full truth.
Suzette Woodward, National Clinical Director, Sign up to Safety Team, NHS England @SuzetteWoodward
Radiographers will say that they adhere to all safety procedures but on occasion they have been known to purposely try to ignore the 6 week post op rule for scanning because to investigate it would delay the list.
Anonymous, Radiographer
Commissioners often use CQUINs (Commissioning for Quality and Innovation payments framework) to drive innovation and quality improvement in the NHS. In theory, the metrics relating to individual CQUINs are agreed between commisioners and clinicians. In practice, some CQUINs focus on meaningless metrics. A hypothetical example: a CQUIN target for treating all patients with a certain diagnosis within an hour of diagnosis is flawed due to a failure of existing coding systems to identify relevant patients. Clinicians inform the commissioners of this major limitation and offer suggested improvements to the metrics. These suggested improvements are not deemed appropriate by the commissioning team because they deviate significantly from previously agreed definitions for the CQUIN. The clinicians are demotivated by the process of collecting meaningless data and are tempted to use gaming solutions to report best performance. This situation is exacerbated by pressure from the management team within the NHS Trust who recognise that failure to demonstrate adherence to the CQUIN key performance indicators is associated with a financial penalty. The management team listen to the clinicians and understand that the data collection is clinically meaningless, but insist that the clinical team collect the data anyway. The motivational driver to improve performance has moved from a desire to improve clinical outcomes to a desire to reduce financial penalties. The additional burden is carried by the clinical team who are expected to collect meaningless data without any additional administrative or job plan support.
Anonymous, NHS paediatrician
In June 2013, David Behan, the new Chief Executive of CQC since 2012, told me that an independent report concluded that an internal CQC report identifying many failures may have been deliberately ‘covered up’. The Grant Thornton report concerned CQC’s regulatory oversight of University Hospitals of Morecambe Bay, an NHS Foundation Trust. David Behan referred us to page 15, paragraph 1.50 of the independent report:
“We have carefully considered whether evidence exists to corroborate the assertion that there was an instruction to delete this report. We conclude that such corroborative evidence exists in the form of a contemporaneous note of the meeting and the lack of action taken on the information included in the report… We were also surprised that the fact that such a review took place and was not shared with us during briefings we held with the senior member of management who allegedly gave the instruction to delete the report, ahead of the commencement of our work. We have given careful consideration to whether the alleged instruction to delete the report could in effect constitute a deliberate ‘cover-up’ and if so what would be the reason for doing so? We have concluded on the balance of the evidence…it might well have constituted a deliberate ‘cover-up’.”
It is one thing when you find out that your local hospital has suffered serious failures in care resulting in numerous preventable deaths, it is another when you find that hospital is involved, if not in blatant cover-up, in obscuring the extent of the problems. But when you find the organisation responsible for regulating hospitals has not only failed to maintain standards but is complicit in its own cover-ups then you can begin to despair whether you will ever get to the bottom of just how and why these tragedies occur.
I had never wanted staff involved in Joshua’s care to be unfairly punished or disciplined over what happened, but I did want them to be honest. I needed the truth to be told including an honest acceptance of the consequences for Joshua and my family. I was not going to accept this cover-up.
James Titcombe, Father of Joshua Titcombe, who died nine days after his birth at Furness General Hospital in Barrow in October 2008, @JamesTitcombe
Healthcare staff often have to complete mandatory online modules, e.g. in fire safety, manual handling, blood transfusion. The modules have a pass rate (e.g. 80%) and sometimes a maximum number of attempts before the healthcare worker is locked out and has to discuss their poor performance with their line manager. Healthcare workers may then sit down in groups to share the correct answers and therefore pass the module.
Anonymous
“Nurses were expected to break the rules as a matter of course in order to meet target, a prime example of this being the maximum four-hour wait time target for patients in A&E. Rather than “breach” the target, the length of waiting time would regularly be falsified on notes and computer records.”
Staff Nurse Donnelly, in ‘Mid Staffordshire NHS Foundation Trust Public Inquiry Vol 1’
The use of checklists for the prevention of Central Line Associated Bacteraemia (CLAB) is well described and has been taken up widely in the healthcare system. The purported benefits of the checklist include ensuring all steps are followed as well as opening up communication between team members. After introducing the CLAB bundle into our Intensive Care Unit, we saw very high levels of reported checklist compliance followed by the expected drop in our rates of infection, confirming the previously reported benefits. However, when we observed our staff it became apparent that they were actually filling in the checklist retrospectively without watching the procedure, as they were busy with other tasks.The fall in the CLAB rate could therefore not have been due to the use of a checklist and instead appears to be due to the use of “CLAB packs”. These put all required items for central line insertion into a single pack thereby making it easier for staff to perform the procedure correctly.
Carl Horsley, Intensivist, @horsleycarl
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. CC BY-NC-ND 4.0
Discover more from Humanistic Systems
Subscribe to get the latest posts sent to your email.

7 thoughts